Recent recommendations state that considerable coronary artery disease (CAD) should be treated before the index procedure in patients with severe aortic stenosis who have a transcatheter aortic valve implant. However, the data supporting this suggestion is still limited. We aimed to assess the recent updates on percutaneous coronary intervention (PCI) among patients undergoing transcatheter aortic valve interventions. A search was performed on the PubMed, Web of Science, Science Direct, EBSCO, SCOPUS, Wiley, and Cochrane Library databases. Study articles were screened by title and abstract using Rayyan QCRI then a full-text assessment was implemented. A total of eleven studies with 6252 patients were included. The self-expandable (SE), balloon-expandable, Edwards Sapien (ES), and CoreValve are the most common valve types used in TAVI or TAVR. Most of the included studies reported that TAVI/ TAVR combined with the PCI technique is a safe and efficacious procedure for managing patients with AS. For patients with severe AS and with or without CAD, combined PCI prior to TAVI/ TAVR is a relatively safe and practical method, according to the available evidence on short- and mid-term results.
INTRODUCTION
Degenerative aortic stenosis (AS) and coronary artery disease (CAD) are two distinct cardiovascular conditions that frequently coexist (Van Hoang et al., 2019). They have many mutual risk factors, pathophysiological mechanisms, and clinical implications (Opolski et al., 2016; El Sabbagh & Nishimura, 2017). Both have a subendothelial buildup of oxidized low-density lipoproteins and inflammatory reactions involving lymphocytes and macrophages, which are factors in the development of the diseases (Otto, 1994; Soboleva et al., 2022).
For patients with severe AS and significant surgical risk, transcatheter aortic valve replacement (TAVR) or transcatheter aortic valve implantation (TAVI) has lately become a desirable and less intrusive treatment option compared to traditional surgical aortic valve replacement (SAVR) (Greason et al., 2014).
It is still debatable how stable CAD should be managed in individuals with aortic stenosis who are undergoing TAVI. There is currently no data demonstrating the prognostic value of undergoing coronary artery revascularization either; prior to, during, or following the TAVI surgery (Ramee et al., 2016; Kotronias et al., 2017). The European Society of Cardiology's most recent myocardial revascularization guidelines advises considering prior PCI for patients undergoing TAVI who have coronary artery stenosis greater than 70% in proximal segments, even though this issue is contentious (Neumann et al., 2019; Sulastri et al., 2022). Similarly, coronary artery revascularization is recommended prior to TAVI, according to the most recent American Society of Cardiology acceptable use criteria (Patel et al., 2017).
This systematic review aims to investigate the recently published literature from 2018 to 2022 on PCI among patients with AS and with/ without CAD and undergoing TAVI or TAVR.
MATERIALS AND METHODS
This systematic review was conducted following the accepted standards (Preferred Reporting Items for Systematic Reviews and Meta-Analyses, PRISMA).
Study design
This was a systematic Review.
Study duration
From November to December 2022.
Study condition
The purpose of this systematic review is to investigate the most recent research within the last five years on PCI in patients with AS, CAD, and undergoing TAVI or TAVR.
Search strategy
A comprehensive literature search was conducted in seven major databases, including PubMed, Web of Science, Science Direct, EBSCO, Scopus, Wiley, and Cochrane Library, to identify the relevant literature. We restricted our search to English and took into account the unique requirements of each database. The following keywords were converted into Mesh terms in PubMed and used to find the appropriate studies; "Percutaneous coronary intervention," "PCI," "Transcatheter aortic valve implantation," "TAVI," "Transcatheter aortic valve replacement," "TAVR," "Coronary artery disease," and "CAD." With the help of the "OR" and "AND" Boolean operators, the appropriate keywords were paired. English-language publications with full texts, freely accessible articles, and human trials were included in the search results.
Selection criteria
Inclusion criteria
The inclusion of the subjects was decided upon based on their relevance to the research, which had the following requirements: male or female patients undergoing PCI and TAVI/ TAVR.
Exclusion criteria
We disregarded all additional publications, ongoing research, and analyses of completed studies that did not concentrate on one of these topics.
Data extraction
When examining the search strategy's results, we used Rayyan (QCRI) to check for duplicates (Ouzzani et al., 2016). The researchers narrowed the combined search results based on a set of inclusion/exclusion criteria to determine the relevance of the titles and abstracts. The reviewers looked at the entire texts of the papers that met the criteria for inclusion. The authors discussed and resolves conflicts in the articles. The approved study was added using a created data extraction form. The authors extracted data about the study titles, authors, study year, study designs, country, population type, participant number, mean age, gender, type of valves, type of approach, success rate, and main outcomes.
Strategy for data synthesis
To provide a qualitative summary of the included study components and outcomes, summary tables made from the data collected from the eligible studies were created. After data extraction for the systematic review, it was decided how to use the included study articles' data best. Studies that met the full-text inclusion criteria but did not provide any data on PCI among patients undergoing TAVI/ TAVR were excluded.
Risk of bias assessment
The standard of the included studies was evaluated using the ROBINS-I risk of bias assessment method for non-randomized trials of treatments (Jüni et al., 2016). Seven different topics were covered: confounding and participant selection for the study, classification of interventions, deviations from intended interventions, missing data, assessment of outcomes, and selection of the reported result.
RESULTS AND DISCUSSION
Search results
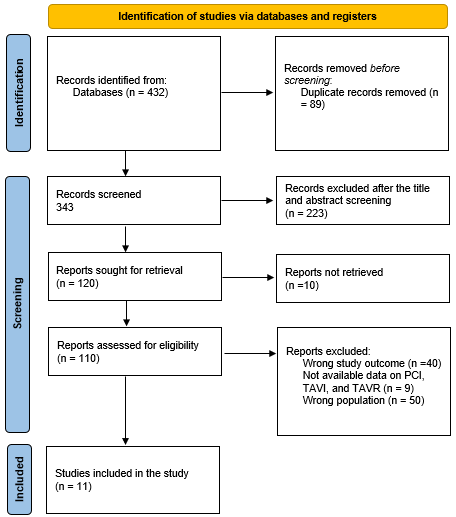
A total of 432 study articles resulted from the systematic search, then 89 duplicates were deleted. Title and abstract screening were conducted on 343 studies, and 223 studies were excluded. 120 reports were sought for retrieval, and only 10 articles were not retrieved. Finally, full-text assessments were performed on the 110 studies; 40 were excluded for wrong study outcomes, 9 for unavailable data on PCI, TAVI, and/ or TAVR, and 50 for the wrong population type. Eleven eligible study articles were included in this systematic review. A summary of the study selection process is presented in Figure 1.
|
|
|
Figure 1. PRISMA flowchart summarizes the study selection process |
Table 1. Sociodemographic characteristics of the participants of the included studies
|
Study |
Country |
Population type |
Participants (n) |
Mean age |
Males (%) |
|
Perrin et al. (2020) |
Switzerland |
Patients with CAD |
19 |
77.7 ± 7.2 |
68.4 |
|
Denimal et al. (2021) |
France |
Patients with and without CAD |
137 |
82.3 ± 6.5 |
38 |
|
Guedeney et al. (2019) |
USA |
Patients with CAD |
81 |
83 ± 7 |
0 |
|
Matta et al. (2021) |
France |
Patients with and without CAD |
1030 |
84.3 ± 7 |
45.2 |
|
Kaihara et al. (2021) |
Japan |
Patients with and without CAD |
186 |
84 ± 6 |
31.7 |
|
Jeroudi et al. (2018) |
USA |
Patients with CAD |
20 |
73.7 ± 12.7 |
55 |
|
Ferreira-Neto et al. (2019) |
Canada |
Patients with CAD |
13 |
70.31 ± 7.99 |
69.2 |
|
Ghrair et al. (2020) |
USA |
Patients with CAD |
852 |
80.5 ±8.3 |
54.1 |
|
Winter et al. (2021) |
Switzerland |
Patients with CAD |
449 |
77-85 |
51.7 |
|
Tran et al. (2022) |
USA |
Patients without CAD |
843 |
80.4 ± 8 |
50.1 |
|
Abugroun et al. (2020) |
USA |
Patients with CAD |
2622 |
74-87 |
52.4 |
Table 2. Characteristics and outcomes of the included studies
|
Study |
Study design |
Type of valve |
Type of approach |
Success rate (%) |
Key findings |
ROBIN-I |
|
Perrin et al. (2020) |
Retrospective study |
CoreValve, Evolut R, Evolut PRO, ES |
TF |
100 |
Even after the installation of a supra-annular SE valve, post-TAV CA and PCI are difficult but doable. High TAVI implantation decreases the need for new pacemaker implantation, but it may make coronary artery cannulation more difficult, particularly if coronary ostia are low. |
High |
|
Denimal et al. (2021) |
Retrospective study |
SE |
TF |
94.2 |
TF-TAVI conducted on a small group of patients entirely under a PCI method has similar efficacy and safety to TF-TAVI performed in the presence of a full anesthetic care team. |
Moderate |
|
Guedeney et al. (2019) |
Prospective study |
SE and balloon-expandable valves |
TF |
NA |
The presence of CAD at baseline, with or without recent PCI, was related to poor 1-year outcomes in women receiving contemporary TAVR. In comparison to patients without CAD, women who underwent PCI within 30 days following TAVR had a higher 1-year risk of death and stroke. |
Moderate |
|
Matta et al. (2021) |
Retrospective study |
SE and balloon-expandable valves |
TF |
NA |
This study offers immediate clinical significance that is helpful in everyday practice. Concomitant CAD and/or preoperative PCI have not been shown to have any deleterious effects on the length of the TAVI hospital stay. |
Moderate |
|
Kaihara et al. (2021) |
Retrospective study |
CoreValve and ES |
TF |
15.6% without complications |
In patients with severe AS treated with TAVI, CAD with an LM or LAD proximal lesion is a potent independent predictor of mid-term major adverse cardiovascular and cerebrovascular events (MACCEs) and all-cause mortality. PCI performed prior to TAVI did not affect the results. |
Moderate |
|
Jeroudi et al. (2018) |
Retrospective study |
CoreValve |
NA |
NA |
The majority of patients with pre-existing CoreValve TAVI can undergo coronary operations successfully. But after TAVI, selective engagement of the RCA ostium proved to be very challenging. |
Moderate |
|
Ferreira-Neto et al. (2019) |
Retrospective study |
Balloon-expandable ES or SAPIEN XT valve |
TF and nontransfemoral |
92.3 |
After TAVR, PCI is possible and can be done without significantly affecting the inserted transcatheter heart valves (THV). |
High |
|
Ghrair et al. (2020) |
Retrospective study |
NA |
Transapical |
NA |
A greater incidence of in-hospital morbidity and mortality was linked to combined TAVR-PCI. |
Moderate |
|
Winter et al. (2021) |
Prospective study |
SE and balloon-expandable valves |
NA |
NA |
In intermediate- and low-risk patients, full revascularization prior to TAVR implantation is a safe and practicable technique. |
Moderate |
|
Tran et al. (2022) |
Retrospective study |
NA |
TF, transaxillary, transaortic, and transaortic |
NA |
In-hospital mortality rates were similar when PCI and TAVR were combined, but rates of acute renal injury were lower, and resource usage was lower. |
Moderate |
|
Abugroun, et al. (2020) |
Retrospective study |
NA |
Transapical |
NA |
While there was no difference in the rate of stroke, TAVR and PCI procedures had greater rates of vascular injury, the requirement for pacemaker implantation, and expense while having lower rates of in-hospital mortality, acute renal injury, sepsis, and shorter lengths of stay. |
Moderate |
Characteristics of the included studies
Table 1 includes the sociodemographic characteristics. All of the included studies comprised patients with underlying CAD except four studies (Denimal et al., 2021; Kaihara et al., 2021; Matta et al., 2021; Tran et al., 2022). A total of 6252 patients were included. Five studies were conducted in the USA (Jeroudi et al., 2018; Guedeney et al., 2019; Abugroun et al., 2020; Ghrair et al., 2020; Tran et al., 2022), two in Switzerland (Winter et al., 2021; Perrin et al., 2022), two in France (Denimal et al., 2021; Matta et al., 2021), one in Japan (Kaihara et al., 2021), and one in Canada (Ferreira-Neto et al., 2019).
Table 2 presents the characteristics of the included studies. Nine studies are retrospective in nature (Ferreira-Neto et al., 2017; Jeroudi et al., 2018; Ghrair et al., 2020; Denimal et al., 2021; Kaihara et al., 2021; Matta et al., 2021; Perrin et al., 2022), and two are prospective studies (Guedeney et al., 2019; Winter et al., 2021). The SE, balloon-expandable, ES, and CoreValve are the most common valve types used in TAVI or TAVR. The transfemoral approach (TF) was the most common approach used. Only three studies reported a clear percentage of the success rate, which ranged from 92.3% (Ferreira-Neto et al., 2019) to 100% (Perrin et al., 2022). One study reported that 15.6% of cases demonstrated a success rate without any complications (Kaihara et al., 2021). The majority of the included studies reported that TAVI/ TAVR combined with the PCI technique is a safe and efficacious procedure for managing patients with AS. A high risk of mortality was reported in three studies (Guedeney et al., 2019; Ghrair et al., 2020; Tran et al., 2022). Complications such as stroke (Guedeney et al., 2019), vascular injury (Abugroun et al., 2020), and hospital morbidity (Ghrair et al., 2020) were recorded.
It is challenging to determine the best method to manage significant aortic stenosis with TAVI/ TAVR. This systematic review included a wide variety of populations undergoing PCI: AS patients with or without CAD, those who used TAVI or TAVR, variable procedure approaches, and numerous valve types. This carries a considerable heterogeneity between studies. Our review is also limited by its lack of a quantitative assessment. Moreover, most of the included studies lacked substantial data, such as the success rates of the applied procedures.
However, we found that the success rate of TAVI or TAVR combined with PCI ranged from 92.3% (Ferreira-Neto et al., 2019) to 100% (Perrin et al., 2022). The pooled periprocedural mortality reported in this review was comparable to the results from sizable, separate TAVI registries (Gilard et al., 2012; Thomas et al., 2012). Additionally, it contrasted favorably with the 9.7% perioperative mortality rate reported after concurrent CABG and SAVR. Concomitant SAVR and CABG, however, have shown to have very good long-term results even in octogenarians, with 1-, 2-, 3-, and 5-year survival rates of 83.2%, 78.8%, 72.9%, and 60.8%, respectively (Vasques et al., 2012).
According to the majority of the papers that were reviewed, managing patients with AS using TAVI/TAVR and the PCI approach is a safe and efficient procedure. These results were consistent with a previous systematic review conducted by Virk et al. (2015). The use of TAVR to treat severe AS in patients who are at high risk for surgery has expanded rapidly and universally over the past several years. Recent studies have also demonstrated TAVR's superior results over SAVR in patients with low to moderate risk. We need to understand how to handle patients with concurrent CAD because TAVR is being increasingly used (Leon et al., 2016). TF-TAVI conducted on a small group of patients entirely under a PCI method has similar efficacy and safety to TF-TAVI performed in the presence of a full anesthetic care team. The PCI technique could be adopted for the majority of TF-TAVI treatments since it seems to be a safe and effective therapeutic pathway that offers an adequate and sensible usage of anaesthesiology resources (Denimal et al., 2021).
We also found a high mortality risk and complications such as stroke (Guedeney et al., 2019), vascular injury (Abugroun et al., 2020), and hospital morbidity (Ghrair et al., 2020; Jamal, 2022) among the target population. Temporary circulatory disturbances during balloon valvuloplasty or rapid ventricular pacing, embolism due to the separation of calcium deposits, and enhanced thrombogenicity brought on by tissue factor release are some of the reasons that may affect stroke and vascular damage in TAVR. There was no major stroke reported in other studies except by Matta et al. (2021), who used SE and balloon-expandable valves
Future studies should concentrate on selecting the most qualified people for pre-TAVI PCI, given the limitations of the existing literature. Quantifying the degree of CAD that indicates pre-TAVI intervention is especially important. To evaluate the relative advantages and dangers of a staged versus concurrent strategy to pre-TAVI PCI, additional research is also necessary. Concurrently performing these two operations in the same location allows for better resource use and the use of a shared artery, but these advantages may be outweighed by the long process and higher contrast burden. Additionally, more clinical data is needed in the case of a staged approach to establish the right interval between the two procedures, the kind of stents to use, and the best anti-platelet regimen. The cost-effectiveness and quality of life following combined PCI and TAVI procedures, both of which are emerging as crucial outcomes for actual clinical application, are currently not covered by any pertinent studies.
CONCLUSION
For patients with severe AS and with or without CAD, combined PCI before TAVI/ TAVR is a relatively safe and practical method, according to the available evidence on short- and mid-term results. However, to choose the best percutaneous treatment plans for individuals with severe AS and concurrent CAD, more randomized controlled trials are required.
ACKNOWLEDGMENTS: Many thanks to Dr. Qaed Salem Alhammami; Assistant Professor and Consultant of radiology, Najran University, Saudi Arabia, for his continuous help, support and encouragement to complete this work.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Abugroun, A., Osman, M., Awadalla, S., & Klein, L. W. (2020). Outcomes of transcatheter aortic valve replacement with percutaneous coronary intervention versus surgical aortic valve replacement with coronary artery bypass grafting. The American Journal of Cardiology, 137, 83-88.
Denimal, T., Delhaye, C., Piérache, A., Robin, E., Modine, T., Moussa, M., Sudre, A., Koussa, M., Debry, N., Pamart, T., et al. (2021). Feasibility and safety of transfemoral transcatheter aortic valve implantation performed with a percutaneous coronary intervention-like approach. Archives of Cardiovascular Diseases, 114(8-9), 537-549.
El Sabbagh, A., & Nishimura, R. A. (2017). Clinical conundrum of coronary artery disease and aortic valve stenosis. Journal of the American Heart Association, 6(2), e005593.
Ferreira-Neto, A. N., Puri, R., Asmarats, L., Vilalta, V., Guimaraes, L., Delarochellière, R., Paradis, J. M., Mohammadi, S., Dumont, E., & Rodés-Cabau, J. (2019). Clinical and technical characteristics of coronary angiography and percutaneous coronary interventions performed before and after transcatheter aortic valve replacement with a balloon-expandable valve. Journal of Interventional Cardiology, 2019, 3579671.
Ghrair, F., Omran, J., Thomas, J., Gifft, K., Eniezat, M., Kumar, A., & Enezate, T. (2020). Outcomes of concomitant percutaneous coronary interventions and transcatheter aortic valve replacement. Archives of Medical Science-Atherosclerotic Diseases, 5(1), 284-289.
Gilard, M., Eltchaninoff, H., Iung, B., Donzeau-Gouge, P., Chevreul, K., Fajadet, J., Leprince, P., Leguerrier, A., Lievre, M., Prat, A., et al. (2012). Registry of transcatheter aortic-valve implantation in high-risk patients. The New England Journal of Medicine, 366(18), 1705-1715.
Greason, K. L., Mathew, V., Suri, R. M., Holmes, D. R., Rihal, C. S., McAndrew, T., Xu, K., Mack, M., Webb, J. G., Pichard, A., et al. (2014). Transcatheter versus surgical aortic valve replacement in patients with prior coronary artery bypass graft operation: A PARTNER trial subgroup analysis. The Annals of Thoracic Surgery, 98(1), 1-8.
Guedeney, P., Tchétché, D., Petronio, A. S., Mehilli, J., Sartori, S., Lefèvre, T., Presbitero, P., Capranzano, P., Iadanza, A., Sardella, G., et al. (2019). Impact of coronary artery disease and percutaneous coronary intervention in women undergoing transcatheter aortic valve replacement: From the WIN-TAVI registry. Catheterization and cardiovascular interventions: Official journal of the Society for Cardiac Angiography & Interventions, 93(6), 1124-1131.
Jamal, B. T. (2022). Does maxillomandibular advancement (MMA) for obstructive sleep apnea (OSA) negatively affect facial appearance? Annals of Dental Specialty, 10(3), 89-92.
Jeroudi, O. M., Rehman, H., & Barker, C. M. (2018). Technical considerations and feasibility of coronary angiography and percutaneous coronary intervention after CoreValve® transcatheter aortic valve implantation. Structural Heart, 2(4), 297-302.
Jüni, P., Loke, Y., Pigott, T., Ramsay, C., Regidor, D., Rothstein, H., Sandhu, L., Santaguida, P. L., Schünemann, H. J., & Shea, B. (2016). Risk of bias in non-randomized studies of interventions (ROBINS-I): Detailed guidance. British Medical Journal, 355, i4919.
Kaihara, T., Higuma, T., Izumo, M., Kotoku, N., Suzuki, T., Kameshima, H., Sato, Y., Kuwata, S., Koga, M., Mitarai, T., et al. (2021). Influence of coronary artery disease and percutaneous coronary intervention on mid-term outcomes in patients with aortic valve stenosis treated with transcatheter aortic valve implantation. Clinical Cardiology, 44(8), 1089-1097.
Kotronias, R. A., Kwok, C. S., George, S., Capodanno, D., Ludman, P. F., Townend, J. N., Doshi, S. N., Khogali, S. S., Généreux, P., Herrmann, H. C., et al. (2017). Transcatheter aortic valve implantation with or without percutaneous coronary artery revascularization strategy: A systematic review and meta‐analysis. Journal of the American Heart Association, 6(6), e005960.
Leon, M. B., Smith, C. R., Mack, M. J., Makkar, R. R., Svensson, L. G., Kodali, S. K., Thourani, V. H., Tuzcu, E. M., Miller, D. C., Herrmann, H. C., et al. (2016). Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. The New England Journal of Medicine, 374(17), 1609-1620.
Matta, A. G., Lhermusier, T., Parada, F. C., Bouisset, F., Canitrot, R., Nader, V., Blanco, S., Elbaz, M., Roncalli, J., & Carrié, D. (2021). Impact of coronary artery disease and percutaneous coronary intervention on transcatheter aortic valve implantation. Journal of Interventional Cardiology, 2021.
Neumann, F. J., Sousa-Uva, M., Ahlsson, A., Alfonso, F., Banning, A. P., Benedetto, U., Byrne, R. A., Collet, J. P., Falk, V., Head, S. J., et al. (2019). 2018 ESC/EACTS guidelines on myocardial revascularization. The task force on myocardial revascularization of the European Society of Cardiology (ESC) and European Association for Cardio-Thoracic Surgery (EACTS). Giornale Italiano di Cardiologia (2006), 20(7-8 Suppl 1), 1S-61S.
Opolski, M. P., Staruch, A. D., Jakubczyk, M., Min, J. K., Gransar, H., Staruch, M., Witkowski, A., Kepka, C., Kim, W. K., Hamm, C. W., et al. (2016). CT angiography for the detection of coronary artery stenoses in patients referred for cardiac valve surgery: Systematic review and meta-analysis. JACC: Cardiovascular Imaging, 9(9), 1059-1070.
Otto, C. M., Kuusisto, J., Reichenbach, D. D., Gown, A. M., & O'Brien, K. D. (1994). Characterization of the early lesion of'degenerative'valvular aortic stenosis. Histological and immunohistochemical studies. Circulation, 90(2), 844-853.
Ouzzani, M., Hammady, H., Fedorowicz, Z., & Elmagarmid, A. (2016). Rayyan—A web and mobile app for systematic reviews. Systematic Reviews, 5(1), 1-10.
Patel, M. R., Calhoon, J. H., Dehmer, G. J., Grantham, J. A., Maddox, T. M., Maron, D. J., & Smith, P. K. (2017). ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate use criteria for coronary revascularization in patients with stable ischemic heart disease: A report of the American college of cardiology appropriate use criteria task force, American association for thoracic surgery, American heart association, American society of echocardiography, American society of nuclear cardiology, society for cardiovascular angiography and interventions, society of cardiovascular computed tomography, and society of thoracic surgeons. Journal of the American College of Cardiology, 69(17), 2212-2241.
Perrin, N., Fassa, A., Baroz, A., Frangos, C., Mock, S., Frei, A., Cimci, M., Degrauwe, S., Roffi, M., Iglesias, J. F., et al. (2022). Complexity assessment and technical aspect of coronary angiogram and percutaneous coronary intervention following transcatheter aortic valve implantation. Cardiology Journal, 29(2), 197-204.
Ramee, S., Anwaruddin, S., Kumar, G., Piana, R. N., Babaliaros, V., Rab, T., Klein, L. W., Aortic Stenosis AUC Writing Group, & Interventional Section of the Leadership Council of the American College of Cardiology (2016). The rationale for performance of coronary angiography and stenting before transcatheter aortic valve replacement: From the interventional section leadership council of the American college of cardiology. JACC: Cardiovascular Interventions, 9(23), 2371-2375.
Soboleva, M. S., Loskutova, E. E., & Kosova, I. V. (2022). Pharmacoepidemiological study of the use of e-pharmacies by the population. Journal of Advanced Pharmacy Education and Research, 12(3), 36-43.
Sulastri, T., Sunyoto, M., Suwitono, M. R., & Levita, J. (2022). The effect of red ginger bread consumption on the physiological parameters of healthy subjects. Journal of Advanced Pharmacy Education and Research, 12(3), 28-35.
Thomas, M., Schymik, G., Walther, T., Himbert, D., Lefèvre, T., Treede, H., Eggebrecht, H., Rubino, P., Colombo, A., Lange, R., et al. (2011). One-year outcomes of cohort 1 in the Edwards SAPIEN Aortic Bioprosthesis European Outcome (SOURCE) registry: The European registry of transcatheter aortic valve implantation using the Edwards SAPIEN valve. Circulation, 124(4), 425-433.
Tran, Z., Hadaya, J., Downey, P., Sanaiha, Y., Verma, A., Shemin, R. J., & Benharash, P. (2022). Staged versus concomitant transcatheter aortic valve replacement and percutaneous coronary intervention: A national analysis. JTCVS Open, 10, 148-161.
Van Hoang, S., Nguyen, K. M., Le Tran, P. U., Mai, L. T., & Tran, H. P. N. (2019). echocardiographic evaluation of elevated left ventricular filling pressures in patients with obstructive coronary artery disease. Archives of Pharmacy Practice, 10(4), 106-13.
Vasques, F., Lucenteforte, E., Paone, R., Mugelli, A., & Biancari, F. (2012). Outcome of patients aged ≥80 years undergoing combined aortic valve replacement and coronary artery bypass grafting: A systematic review and meta-analysis of 40 studies. American Heart Journal, 164(3), 410-418.
Virk, S. A., Tian, D. H., Liou, K., Pathan, F., Villanueva, C., Akhunji, Z., & Cao, C. (2015). Systematic review of percutaneous coronary intervention and transcatheter aortic valve implantation for concomitant aortic stenosis and coronary artery disease. International Journal of Cardiology, 187, 453-455.
Winter, M. P., Hofbauer, T. M., Bartko, P. E., Nitsche, C., Koschutnik, M., Kammerlander, A. A., Donà, C., Spinka, G., Spinka, F., Andreas, M., et al. (2021). Clinical impact of pre-procedural percutaneous coronary intervention in low- and intermediate-Risk transcatheter aortic valve replacement recipients. Journal of Personalized Medicine, 11(7), 633.
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.