Aortic dissection is a rare occurrent condition involving the body’s main artery, the aorta, and carrying with it high morbidity and mortality. It is one of the conditions that fall under the term acute aortic syndromes. Although it is uncommon, it is hard to describe the true number of cases as most cases are based on autopsy reports. Therefore, to encounter this catastrophic condition, early diagnosis and immediate management are vital for the survival of patients. The goal was to review the literature to enhance the awareness and understanding of mesenteric ischemia. We reviewed the literature for aortic dissection; pathophysiology, classification, diagnosis, and options for treatment. Articles were selected from the PubMed database, and the studies selected were subjected to a thorough review. Aortic dissection is an uncommon condition presenting as severe chest or back pain. Although it is uncommon, it remains a potentially fatal condition that may jeopardize a patient’s life. It starts with a tear in the aortic intima, that can propagate on both sides leading eventually to end-organ ischemia and death. Early diagnosis and rapid management are the keys to a patient’s survival.
INTRODUCTION
Thoracic aortic dissection is a catastrophic consequential manifestation of the acute aortic syndrome, leading to high morbidity and mortality worldwide. It is a serious condition involving the major artery of the body, the aorta. The process of this condition takes place when a tear in the innermost layer of the thoracic aortic wall, called intima, causes the blood to flow amidst the layers of the wall, forcing the layers to split apart (Hagan et al., 2000; Al Abusaab et al., 2019; Mohamed et al., 2019). Although roughly uncommon, it is still deemed a life-threatening condition that may jeopardize a patient’s life. The incidence in the United States is estimated to range from 3-4 cases per 100,000 per year according to literature (Clouse et al., 2004; Patel & Arora, 2008). Nevertheless, it is hard to measure the true frequency as most estimates are founded on autopsy studies. This is because a considerable number of patients pass away either before arriving at the hospital or before the condition gets identified (Olsson et al., 2006). Autopsy studies have shown evidence of aortic dissection to be estimated between 1-3% of all autopsies (Clouse et al., 2004). Aortic dissection is more frequent in males than females with a ratio of 2-3:1, and around 75% of dissections occur in people between the ages of 40 and 70, with a peak between the ages of 50 and 65 (Patel & Arora, 2008).
Interestingly, the incidence is predicted to be increasing over time, owing to the advancement of diagnostic imaging and screening programs. However, it remains a catastrophic condition posing high morbidity and mortality. Therefore, early diagnosis and prompt management are vital for the survival of patients (Olsson et al., 2006; Tsai et al., 2006). In this review, we discuss the different classifications of aortic dissection, pathophysiology, diagnosis, and treatment.
MATERIALS AND METHODS
We used the PubMed database for the process of selecting relevant articles, and the following keys used in the mesh ((“Aortic Dissection"[Mesh]) OR (“Pathophysiology"[Mesh] OR "Classification"[Mesh] OR "Diagnosis"[Mesh] OR "Treatment"[Mesh])). For the inclusion criteria, the articles were chosen according to one of the following: Aortic dissection or Aortic dissection’s pathophysiology, classification, diagnosis, and treatment. Exclusion criteria were all other articles that did not meet the criteria because they did not have any results of the inclusion criteria in their topic.
Classification
The anatomy of the thoracic aorta consists of the ascending aorta, transverse aortic arch, and descending thoracic aorta. The ascending aorta is further divided into two parts: the aortic root, and a tubular part. The transverse aortic arch gives rise to the brachiocephalic arteries. The descending thoracic aorta starts distal to the left subclavian artery and runs to the diaphragm (Dagenais, 2011). The parts that are implicated in the Thoracic Aortic Dissection (TAD) are the proximal segments (the ascending aorta and transverse aortic arch), the distal segment (the descending thoracic aorta), or both segments (Nienaber & Eagle, 2003). Knowing the anatomy of the thoracic aorta is very important in this condition, as the classification is based on its anatomy. TAD can also be classified based on its etiology.
Anatomic classification
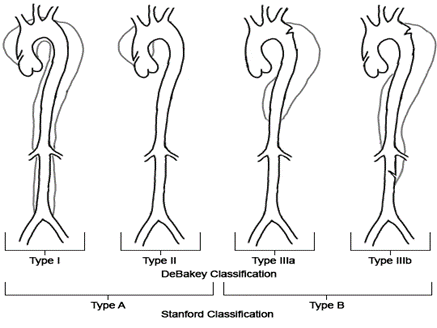
Two anatomical classifications are commonly in use for TAD: the DeBakey system, and the Stanford system, see Figure 1. the Stanford system classifies TAD as type A for dissections that involve ascending aorta; regardless of the primary intimal tear site, and all other dissections are classified as type B. On the other hand, the DeBakey system categorizes TAD based on the site of primary intimal tear as follows: type 1 originates in the ascending aorta and extends to the aortic arch, type 2 originates in and is restricted to the ascending aorta, and type 3 arises in the descending aorta and extends proximally or distally but not beyond the left subclavian artery (Daily, 1970; Nienaber & Eagle, 2003; Tsai et al., 2005).
|
|
|
Figure 1. Aortic Dissection Anatomical Calssification |
Etiological classification
Traumatic: Thoracic aortic dissection can be caused by a physical injury mechanism or might be iatrogenic due to instrumentation, such as in catheterization, or dissection following aortic repair (Khandheria et al., 1989; Blanchard et al., 1994; Januzzi et al., 2004).
Degenerative: Aortic dissection with a degenerative origin has not been linked to any recognized genetically induced disorders (Clouse et al., 2004).
Genetical: some syndromes are associated with aortic dissection, such as Marfan syndrome, Ehlers-Danlos syndrome, Loeys-Dietz syndrome, and Turner syndrome. Moreover, it is associated with non-syndromic conditions, such as familial TAAD or bicuspid aortic valve (Roberts & Roberts, 1991; Ptaszek et al., 2015; Isselbacher et al., 2016; Chen et al., 2020).
Variants
Aortic dissection also has numerous variants that fall under the term “Acute Aortic Syndromes”. These include aortic intramural hematoma, intimal tear without hematoma, and penetrating atherosclerotic ulcer (Nienaber et al., 2004; Tsai et al., 2005).
Pathophysiology
The originating event for aortic dissection is intimal tear, which can be preceded by degenerative process or cystic medial necrosis in cases of nontraumatic aortic dissection. When the tear occurs, the blood passes through the tear leading to separation of the intima from the media and/or adventitia enveloping the intima, resulting in the creation of false lumen. It's unclear if the first event is a rudimentary rupture of the intima with subsequent media dissection or a hemorrhage inside the media with later intima rupture (Larson & Edwards, 1984).
More than half of all aortic intimal tears start in the ascending aorta at the sino-tubular junction and spread throughout the rest of the thoracoabdominal aorta. Furthermore, around 20 to 30 percent of tears begin at the left subclavian artery and spread into the descending thoracic and thoracoabdominal aorta (Hagan et al., 2000). It is speculated that these two locations are common due to shear forces being highest in them (Hirst et al., 1958; Crawford, 1990).
The dissection can spread proximally or distally, Involving the aortic valve and the pericardial space or branching vessels. Many ischemic clinical conditions, such as cardiac tamponade, aortic regurgitation, or ischemia of different locations in the body, are caused by this propagation (Nienaber & Eagle, 2003). Patients with ascending aortic involvement are at high risk of aortic rupture. The intimal tear caused by type B dissection can whorl into a cleavage plane within the media of the aorta together with the posterolateral descending thoracic aorta, rendering the celiac, superior mesenteric, and right renal arteries in the true lumen and the left renal artery in the false lumen (Crawford, 1990). Disparities in dissection anatomy are common, highlighting the importance of appropriate axial imaging. Furthermore, numerous communications between the true and fake lumens may emerge (Nienaber & Eagle, 2003).
The true lumen collapses to a varying degree and the false lumen dilates right after dissection, thus leading to an increase in the cross-sectional area of the aorta. Blood pressure, the size of the entry tear into the false lumen, the depth of the dissection plane inside the media, and the proportion of aortic circumference implicated all affect the increase of false lumen area. Because the fake lumen's outer wall is thinned, it expands to create the wall tension required to withstand aortic pressure. The cause of the collapse of the true lumen is the pressure difference between the true and false lumens, which is worsened by the intrinsic rebound of the muscle components inside the dissection flap (Williams et al., 1997; Nakagawa et al., 2021).
Because the dissection can spread across the thoracoabdominal aorta, mal-perfusion of aortic branch arteries may ensue. Avascular beds can be mal-perfused in one or more branch regions at the same time. "Dynamic obstruction" and "static obstruction" are the terms used to describe the processes of aortic branch vessels ma-perfusion (Williams et al., 1997; Suhartati et al., 2021). Mal-perfusion syndromes are found in 30 to 45 percent of descending dissections and are linked to an increased risk of early death (Cambria et al., 1988; Hagan et al., 2000; Lauterbach et al., 2001).
Clinical presentation
Symptoms and signs
Acute pain — Pain is the most frequent presenting symptom, affecting over 90% of patients, with the majority reporting a sudden onset. The pain is described as intense and sharp, prompting the patient to seek medical help within minutes to hours after the start, and is unlike any agony he or she has ever felt. Pain can be present alone or in conjunction with other clinical symptoms or signs such as syncope, acute coronary syndrome, cerebrovascular accident, or heart failure (Pape et al., 2015; Evangelista et al., 2018). Although uncommon, non-painless dissections have been reported, commonly in patients older than 60 years with ascending aortic dissection (Park et al., 2004).
While the pain in ascending (type A) dissection is often described as anterior chest pain, the pain in descending (type B) dissection is more commonly described as being in the back. Generally, type A dissection patients experience chest pain more frequently than type B, while back pain and abdominal pain are experienced more in type B (Hagan et al., 2000; Pape et al., 2015). For radiation, the pain can radiate anywhere in the thorax and abdomen (Larson & Edwards, 1984; Hagan et al., 2000; Evangelista et al., 2018). Typical symptoms of aortic dissection are substantially less frequent in those over 70 years of age and were less probably to have a sudden onset of pain than younger patients (Mehta et al., 2002; Evangelista et al., 2018).
Pulse deficit — the presence of reduced or absent blood flow to peripheral arteries manifests as a pulse deficit, which is described as a weak or nonexistent carotid, brachial, or femoral pulse caused by an intimal flap or hematoma pressure. In patients suffering from an aortic dissection, a significant difference (>20 mmHg) in systolic blood pressure may be seen. Comparatively, females appear to be less likely to have pulse deficit than males, and older patients are less likely to have it than younger patients (Mehta et al., 2002; Nienaber et al., 2004). Notably, some studies have associated the presence of pulse deficit with high mortality. When compared to patients without a pulse deficit, those with a pulse deficit had a greater incidence of in-hospital adverse events and death (Bossone et al., 2002; Nallamothu et al., 2002).
Valvular murmur — The aortic valve can be involved in aortic dissections that spread proximally from the original tear (Nienaber & Eagle, 2003). A novel diastolic murmur is a sign that comes along with severe chest pain in acute aortic regurgitation. It is a diastolic decrescendo murmur that is usually associated with wide pulse pressure, hypotension, and/or heart failure. Acute aortic valve regurgitation develops in up to two-thirds of ascending dissections (Hagan et al., 2000; Movsowitz et al., 2000).
Neurologic deficit — Focal neurologic impairments can occur as a result of dissection propagation involving branch arteries proximally or distally from the original tear, or as a result of mass effects when the expanding aorta compresses adjacent tissues (Nienaber et al., 2004). As a consequence, the patient may develop stroke, altered consciousness, Horner’s syndrome, or acute paraplegia (Hagan et al., 2000; Aktas et al., 2008).
Hypotension — Individuals with ascending aortic dissection are more likely to experience syncope, hypotension, and/or shock at first presentation, whilst individuals with descending aortic dissection are more likely to have hypertension (Nallamothu et al., 2002). Hypotension and shock may be caused by aortic rupture or dissection propagation. They can be attributed to cardiac tamponade, aortic valve regurgitation, myocardial infarction, hemothorax, or hemoperitoneum (Nienaber et al., 2004).
Diagnostic plan
To avoid a missing or delayed diagnosis, it's critical to have a high index of suspicion when detecting individuals with acute aortic dissection. Acute ascending thoracic aortic dissection, which is a cardiac surgical emergency, must be distinguished quickly from descending thoracic aortic dissection, which is treated medically in hemodynamically stable patients without end-organ compromise (Hansen et al., 2007; Chua et al., 2012; Huynh et al., 2019; Parvez et al., 2021). Generally, conclusive vascular imaging investigations should not be done on a patient until they have been stabilized. Recognizing the clinical triad of aortic dissection may aid in identifying the condition, which includes sudden onset of sharp or tearing thoracic or abdominal pain, variation in pulse and/or blood pressure, and mediastinal widening evident on chest radiograph (von Kodolitsch et al., 2000).
Chest radiograph
Chest radiographs are routinely acquired to assist in quickly distinguishing between the various causes of chest discomfort, such as pneumothorax. Widening of the mediastinum or aortic silhouette is the most frequent abnormalities detected by chest x-ray (Hagan et al., 2000; von Kodolitsch et al., 2004). Widening of the aorta contour, calcification, aortic kinking, and opacification of the aorticopulmonary window, and hemothorax are among other signs that are less specific for dissection but have been documented (von Kodolitsch et al., 2004).
Laboratory tests
Serum markers for acute aortic dissection are being more often used as a diagnostic tool, particularly for distinguishing chest pain in individuals with for whom extensive cardiovascular imaging would be prohibitively expensive (Suzuki et al., 2009).
D-dimer: The serum marker D-dimer has been identified as a possible marker for acute dissection. D-dimer. Nevertheless, it can be increased in a variety of conditions rendering it a nonspecific indicator of intravascular coagulation (Suzuki et al., 2009; Asha & Miers, 2015). With a threshold of 500 ng/mL, D-dimer appears to be a helpful screening tool for identifying patients who do not have acute aortic dissection. A level lower than this one is extremely indicative of the absence of dissection (Suzuki et al., 2009).
Other tests: smooth muscle myosin heavy chain, soluble ST2, soluble elastin fragments, C-reactive protein, fibrinogen, and fibrillin are among the several experimental tests available (Suzuki et al., 1996; Suzuki et al., 2010; Akutsu et al., 2016; Wang et al., 2018).
Diagnostic imaging
Computed tomographic (CT) angiography, magnetic resonance (MR) angiography, and multiplane transesophageal echocardiography (TEE) are some of the imaging modalities that may be utilized to visualize the dissection. Each has upsides and downsides, and one may be more suited as initial imaging for certain patients (Kienzl et al., 2012). Due to its broad availability, CT is the most usual first choice, particularly in the emergency department. The presence of an intimal flap separating the false lumen from the true lumen, as well as imaging evidence of related abnormalities or complications, are used to diagnose aortic dissection (Moon et al., 2011; Sueyoshi et al., 2013; Mark et al., 2019).
Hemodynamically unstable patients — Transesophageal echocardiography (TEE) as initial imaging is recommended for hemodynamically unstable patients or those with clinical characteristics indicative of ascending aortic dissections. It is reported to have a high sensitivity and specificity. Moreover, it has the advantage of being widely available, and easy to use at the bedside (Nienaber et al., 1993; Moore et al., 2002). Imaging-wise, TEE can reveal tear entry sites, flow or thrombus of the fake lumen, implication of the arch or coronary artery, varying degrees of valve regurgitation, and pericardial effusions. TEE has the drawback of requiring esophageal intubation, which typically necessitates procedural sedation, which may have unfavorable consequences in hemodynamically unstable individuals. Another disadvantage is that to achieve reliable findings, TEE necessitates the availability of experienced operators (Hartnell et al., 1993). Regardless of these limitations, TEE can be very effective in identifying acute dissection and pertinent surgical disease in the ascending aorta, and it is thus primarily used in this area (Nienaber et al., 1993).
Hemodynamically stable patients — CT angiography is an excellent initial study to perform in patients with suspected aortic dissection, who are hemodynamically stable and do not have clinical features suggesting ascending aortic involvement, particularly in the emergency department setting where other studies are limited. The vast majority of patients with suspected acute aortic dissection should have dynamic contrast-enhanced fine-cut CT scan of the chest and abdomen performed (Nienaber et al., 1993). CT angiography is the least operator-dependent modality, offers important anatomic correlations for surgical and endovascular treatment, and captures data for follow-up use. Most significantly, three-dimensional CT scan reconstructions imaging can help with treatment planning, and axial imaging provides the best chance to discover topographic connections between the true and false lumens as well as possible aortic branch impairment (LePage et al., 2001).
Immediate care and treatment
Patients suspected to have aortic dissection should be quickly admitted to the intensive care unit after confirming the diagnosis for the sake of pain control with morphine and anti-impulse medications. Moreover, a toxicology screen should be performed for any case that presents with the acute aortic syndrome, especially if no other known risk factors exist. Toxicology test findings may influence the pharmacological drugs used for acute medical treatment (Erbel et al., 2001; Tsai et al., 2005). Blood pressure monitoring using arterial access is usually required for patients to control changes in blood pressure as quickly as possible. Patients who are unstable or do not have a patent airway should be intubated. Acute medicinal treatments should not obstruct prompt transport to the operating room for individuals who require emergency surgery (Chan et al., 2014).
Anti-impulse therapy
The objective of anti-impulse treatment is to lower the speed at which the left ventricular contraction works, therefore lowering shear stress and slowing the development of the lesion. The first line of therapy is usually a beta-blocker given in the intravenous route to keep the heart rate below 60 beats per minute. It also aids in reducing the systolic blood pressure to the lowest level sustained without impairing mental status or urine production, which is usually between 100 and 120 mmHg (Trimarchi et al., 2010; Di Eusanio et al., 2013). Because of its short half-life and ability to titrate the effect, esmolol is chosen in the acute situation. Moreover, it is a good choice for patients with contraindications to beta-blocker use, such as asthma or heart failure. In individuals who cannot tolerate beta-blockers, diltiazem or verapamil are alternative options (Tsai et al., 2005).
Intervention
Open surgical and endovascular treatment
The location of the affected aorta and the occurrence of complications determine the course of treatment for acute aortic syndromes. Type A dissections are often treated with early surgery, but type B may often be managed with continuous medical treatment. Generally, open surgical methods are used to correct type A aortic lesions, but an initial endovascular approach is appropriate for most type B aortic lesions, providing the patient's anatomy allows for endograft insertion (Nienaber & Eagle, 2003; Tsai et al., 2005). Aortic dissection of type A is a surgical emergency, and rupture of the dissected aorta is relatively uncommon, but it is a serious complication with a high death rate unless immediate surgical intervention is performed. The occurrence of mal-perfusion in this type is linked to a high mortality rate (Geirsson et al., 2007; Di Eusanio et al., 2013; Pacini et al., 2013).
Medical treatment is used to treat the majority of lesions associated with acute aortic syndromes affecting the descending aorta (type B). Intervention, whether surgical or endovascular, is often reserved for patients with severe hypertension, obstinate or recurring pain, propagation of dissection, aneurysmal enlargement, mal-perfusion resulting in organ ischemia, or rupture (Tsai et al., 2005).
Follow-Up
For patients who are not receiving the urgent intervention, follow-up with clinical examinations and vascular imaging, either CT, MR angiography, are done at the interval of 1, 3, 6, and 12 months. Thereafter, it is conducted in a yearly interval to identify mal-perfusions or aneurysm development. Similarly, patients who have had surgery or endovascular repair are followed accordingly (Li et al., 2019).
CONCLUSION
Aortic dissection is a rare condition that frequently manifests as a life-threatening disease with significant chest or back pain and severe hemodynamic compromise. The triggering event is a tear in the intima of the aorta, leading to the development of severe pain. Furthermore, the dissection can propagate in both directions, resulting ultimately in end-organ ischemia and death. For survival, it's critical to have a proper diagnosis and treatment as soon as possible. Options of intervention, either open or endovascular procedure, are chosen according to the type of dissection in terms of site, patient’s profile, and associated complications.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Aktas, C., Cınar, O., Ay, D., Gürses, B., & Hasmanoglu, H. (2008). Acute aortic dissection with painless paraplegia: Report of 2 cases. The American Journal of Emergency Medicine, 26(5), 631-e3. doi:10.1016/J.AJEM.2007.09.020
Akutsu, K., Yamanaka, H., Katayama, M., Yamamoto, T., Takayama, M., Osaka, M., Sato, N., & Shimizu, W. (2016). Usefulness of measuring the serum elastin fragment level in the diagnosis of an acute aortic dissection. The American Journal of Cardiology, 118(9), 1405-1409. doi:10.1016/J.AMJCARD.2016.07.052
Al Abusaab, A. H., Alamri, A. A., Altheyab, A. S., Alqahtani, R. M., Alahdal, E. T., Alofui, E. A., Bokhamseen, H. A., Mobarki, W. M., Aldawsari, W. M., & Aljifry, S. K. A. (2019). Evolution role of imaging techniques in diagnosis and management of pulmonary embolism. Archives of Pharmacy Practice, 10(1), 15-8.
Asha, S. E., & Miers, J. W. (2015). A systematic review and meta-analysis of D-dimer as a rule-out test for suspected acute aortic dissection. Annals of Emergency Medicine, 66(4), 368-378. doi:10.1016/J.ANNEMERGMED.2015.02.013
Blanchard, D. G., Kimura, B. J., Dittrich, H. C., & DeMaria, A. N. (1994). Transesophageal echocardiography of the aorta. Jama, 272(7), 546-551. doi:10.1001/JAMA.1994.03520070066040
Bossone, E., Rampoldi, V., Nienaber, C. A., Trimarchi, S., Ballotta, A., Cooper, J. V., Smith, D. E., Eagle, K. A., & Mehta, R. H. (2002). Usefulness of pulse deficit to predict in-hospital complications and mortality in patients with acute type A aortic dissection. The American Journal of Cardiology, 89(7), 851-855. doi:10.1016/S0002-9149(02)02198-7
Cambria, R. P., Brewster, D. C., Gertler, J., Moncure, A. C., Gusberg, R., Tilson, M. D., Darling, R. C., Hammond, G., Megerman, J., & Abbott, W. M. (1988). Vascular complications associated with spontaneous aortic dissection. Journal of Vascular Surgery, 7(2), 199-209. Accessed September 4, 2021. https://pubmed-ncbi-nlm-nih-gov.ezproxy.alfaisal.edu/3276932/
Chan, K. K., Lai, P., & Wright, J. M. (2014). First‐line beta‐blockers versus other antihypertensive medications for chronic type B aortic dissection. Cochrane Database of Systematic Reviews, 2014(2). doi:10.1002/14651858.CD010426.PUB2
Chen, S. W., Kuo, C. F., Huang, Y. T., Lin, W. T., Chien-Chia Wu, V., Chou, A. H., Lin, P. J., Chang, S. H., & Chu, P. H. (2020). Association of family history with incidence and outcomes of aortic dissection. Journal of the American College of Cardiology, 76(10), 1181-1192. doi:10.1016/J.JACC.2020.07.028
Chua, M., Ibrahim, I., Neo, X., Sorokin, V., Shen, L., & Ooi, S. B. (2012). Acute aortic dissection in the ED: Risk factors and predictors for missed diagnosis. The American Journal of Emergency Medicine, 30(8), 1622-1626. doi:10.1016/J.AJEM.2011.11.017
Clouse, W. D., Hallett, J. W., Schaff, H. V., Spittell, P. C., Rowland, C. M., Ilstrup, D. M., & Melton III, L. J. (2004). Acute aortic dissection: Population-based incidence compared with degenerative aortic aneurysm rupture. In Mayo Clinic Proceedings, 79(2), 176-180. Elsevier. doi:10.4065/79.2.176
Crawford, E. S. (1990). The diagnosis and management of aortic dissection. Jama, 264(19), 2537-2541. doi:10.1001/JAMA.1990.03450190069031
Dagenais, F. (2011). Anatomy of the thoracic aorta and of its branches. Thoracic Surgery Clinics, 21(2), 219-227. doi:10.1016/J.THORSURG.2010.12.004
Daily, P. O. (1970). Management of acute aortic dissections. The Annals of Thoracic Surgery, 10(3), 237-247. doi:10.1016/S0003-4975(10)65594-4
Di Eusanio, M., Trimarchi, S., Patel, H. J., Hutchison, S., Suzuki, T., Peterson, M. D., Di Bartolomeo, R., Folesani, G., Pyeritz, R. E., Braverman, A. C., et al. (2013). Clinical presentation, management, and short-term outcome of patients with type A acute dissection complicated by mesenteric malperfusion: Observations from the international registry of acute aortic dissection. The Journal of Thoracic and Cardiovascular Surgery, 145(2), 385-390. doi:10.1016/J.JTCVS.2012.01.042.
Erbel, R., Alfonso, F., Boileau, C., Dirsch, O., Eber, B., Haverich, A., Rakowski, H., Struyven, J., Radegran, K., Sechtem, U., et al. (2001). Diagnosis and management of aortic dissection: Task force on aortic dissection, European society of cardiology. European Heart Journal, 22(18), 1642-1681. doi:10.1053/EUHJ.2001.2782
Evangelista, A., Isselbacher, E. M., Bossone, E., Gleason, T. G., Eusanio, M. D., Sechtem, U., Ehrlich, M. P., Trimarchi, S., Braverman, A. C., Myrmel, T., et al. (2018). Insights from the international registry of acute aortic dissection: A 20-year experience of collaborative clinical research. Circulation, 137(17), 1846-1860. doi:10.1161/CIRCULATIONAHA.117.031264
Geirsson, A., Szeto, W. Y., Pochettino, A., McGarvey, M. L., Keane, M. G., Woo, Y. J., Augoustides, J. G., & Bavaria, J. E. (2007). Significance of malperfusion syndromes prior to contemporary surgical repair for acute type A dissection: Outcomes and need for additional revascularizations. European Journal of Cardio-Thoracic Surgery, 32(2), 255-262. doi:10.1016/J.EJCTS.2007.04.012
Hagan, P. G., Nienaber, C. A., Isselbacher, E. M., Bruckman, D., Karavite, D. J., Russman, P. L., Evangelista, A., Fattori, R., Suzuki, T., Oh, J. K., et al. (2000). The international registry of acute aortic dissection (IRAD): New insights into an old disease. Jama, 283(7), 897-903. doi:10.1001/JAMA.283.7.897
Hansen, M. S., Nogareda, G. J., & Hutchison, S. J. (2007). Frequency of and inappropriate treatment of misdiagnosis of acute aortic dissection. The American Journal of Cardiology, 99(6), 852-856. doi:10.1016/J.AMJCARD.2006.10.055
Hartnell, G., Costello, P., Goldstein, S. A., Lindsay, J., Vasan, R., Nienaber, C. A., Spielmann, R. P., Cigarroa, J. E., Eagle, K. A., & Isselbacher, E. M. (1993). The diagnosis of thoracic aortic dissection by noninvasive imaging procedures. New England Journal of Medicine, 328(22), 1637-1638. doi:10.1056/NEJM199306033282213
Hirst Jr, A. E., Johns Jr, V. J., & Kime Jr, S. W. (1958). Dissecting aneurysm of the aorta: A review of 505 cases. Medicine, 37(3), 217-279. doi:10.1097/00005792-195809000-00003
Huynh, N., Thordsen, S., Thomas, T., Mackey-Bojack, S. M., Duncanson, E. R., Nwuado, D., Garberich, R. F., & Harris, K. M. (2019). Clinical and pathologic findings of aortic dissection at autopsy: Review of 336 cases over nearly 6 decades. American Heart Journal, 209, 108-115. doi:10.1016/J.AHJ.2018.11.006
Isselbacher, E. M., Lino Cardenas, C. L., & Lindsay, M. E. (2016). Hereditary influence in thoracic aortic aneurysm and dissection. Circulation, 133(24), 2516-2528. doi:10.1161/CIRCULATIONAHA.116.009762
Januzzi, J. L., Isselbacher, E. M., Fattori, R., Cooper, J. V., Smith, D. E., Fang, J., Eagle, K. A., Mehta, R. H., Nienaber, C. A., & Pape, L.A. (2004). Characterizing the young patient with aortic dissection: Results from the International registry of aortic dissection (IRAD). Journal of the American College of Cardiology, 43(4), 665-669. doi:10.1016/J.JACC.2003.08.054
Khandheria, B. K., Tajik, A. J., Taylor, C. L., Safford, R. E., Miller Jr, F. A., Stanson, A. W., Sinak, L. J., Oh, J. K., & Seward, J. B. (1989). Aortic dissection: Review of value and limitations of two-dimensional echocardiography in a six-year experience. Journal of the American Society of Echocardiography, 2(1), 17-24. doi:10.1016/S0894-7317(89)80025-2
Kienzl, D., Prosch, H., Töpker, M., & Herold, C. (2012). Imaging of non-cardiac, non-traumatic causes of acute chest pain. European Journal of Radiology, 81(12), 3669-3674. doi:10.1016/J.EJRAD.2011.02.042
Larson, E. W., & Edwards, W. D. (1984). Risk factors for aortic dissection: A necropsy study of 161 cases. The American Journal of Cardiology, 53(6), 849-855. doi:10.1016/0002-9149(84)90418-1
Lauterbach, S. R., Cambria, R. P., Brewster, D. C., Gertler, J. P., LaMuraglia, G. M., Isselbacher, E. M., Hilgenberg, A. D., & Moncure, A. C. (2001). Contemporary management of aortic branch compromise resulting from acute aortic dissection. Journal of Vascular Surgery, 33(6), 1185-1192. doi:10.1067/MVA.2001.115377
LePage, M. A., Quint, L. E., Sonnad, S. S., Deeb, G. M., & Williams, D. M. (2001). Aortic dissection: CT features that distinguish true lumen from false lumen. American Journal of Roentgenology, 177(1), 207-211. doi:10.2214/AJR.177.1.1770207
Li, Z., Lu, B., Chen, Y., Hou, Z., Chen, B., Zhang, Y., An, Y., & Wei, Y. (2019). Acute type B aortic intramural hematoma: The added prognostic value of a follow-up CT. European Radiology, 29(12), 6571-6580. doi:10.1007/S00330-019-06254-0
Mark, D. G., Davis, J. A., Hung, Y. Y., & Vinson, D. R. (2019). Discriminatory value of the ascending aorta diameter in suspected acute type A aortic dissection. Academic Emergency Medicine, 26(2), 217-225. doi:10.1111/ACEM.13547
Mehta, R. H., O’Gara, P. T., Bossone, E., Nienaber, C. A., Myrmel, T., Cooper, J. V., Smith, D. E., Armstrong, W. F., Isselbacher, E. M., Pape, L. A., et al. (2002). Acute type A aortic dissection in the elderly: Clinical characteristics, management, and outcomes in the current era. Journal of the American College of Cardiology, 40(4), 685-692. doi:10.1016/S0735-1097(02)02005-3
Mohamed, A. M., Badr, N. M., Hagag, A. A., & Mohamed, Y. M. (2019). Intra versus extra-thoracic oscillations in chronic obstructive pulmonary disease (a randomized clinical trial). Journal of Advanced Pharmacy Education and Research, 9(3), 85-90.
Moon, M. C., Greenberg, R. K., Morales, J. P., Martin, Z., Lu, Q., Dowdall, J. F., & Hernandez, A. V. (2011). Computed tomography-based anatomic characterization of proximal aortic dissection with consideration for endovascular candidacy. Journal of Vascular Surgery, 53(4), 942-949. doi:10.1016/J.JVS.2010.10.067
Moore, A. G., Eagle, K. A., Bruckman, D., Moon, B. S., Malouf, J. F., Fattori, R., Evangelista, A., Isselbacher, E. M., Suzuki, T., Nienaber, C. A., et al. (2002). Choice of computed tomography, transesophageal echocardiography, magnetic resonance imaging, and aortography in acute aortic dissection: International registry of acute aortic dissection (IRAD). American Journal of Cardiology, 89(10), 1235-1238. doi:10.1016/S0002-9149(02)02316-0
Movsowitz, H. D., Levine, R. A., Hilgenberg, A. D., & Isselbacher, E. M. (2000). Transesophageal echocardiographic description of the mechanisms of aortic regurgitation in acute type A aortic dissection: Implications for aortic valve repair. Journal of the American College of Cardiology, 36(3), 884-890. doi:10.1016/S0735-1097(00)00766-X
Nakagawa, N., Odanaka, K., Ohara, H., & Kisara, S. (2021). Evaluation of drug information literacy gained through e-learning to prepare students for practical pharmacy experience. Journal of Advanced Pharmacy Education and Research, 11(4), 111-115.
Nallamothu, B. K., Mehta, R. H., Saint, S., Llovet, A., Bossone, E., Cooper, J. V., Sechtem, U., Isselbacher, E. M., Nienaber, C. A., Eagle, K. A., et al. (2002). Syncope in acute aortic dissection: Diagnostic, prognostic, and clinical implications. The American Journal of Medicine, 113(6), 468-471. doi:10.1016/S0002-9343(02)01254-8
Nienaber, C. A., & Eagle, K. A. (2003). Aortic dissection: New frontiers in diagnosis and management: Part I: From etiology to diagnostic strategies. Circulation, 108(5), 628-635. doi:10.1161/01.CIR.0000087009.16755.E4
Nienaber, C. A., Fattori, R., Mehta, R. H., Richartz, B. M., Evangelista, A., Petzsch, M., Cooper, J. V., Januzzi, J. L., Ince, H., Sechtem, U., et al. (2004). Gender-related differences in acute aortic dissection. Circulation, 109(24), 3014-3021. doi:10.1161/01.CIR.0000130644.78677.2C
Nienaber, C. A., von Kodolitsch, Y., Nicolas, V., Siglow, V., Piepho, A., Brockhoff, C., Koschyk, D. H., & Spielmann, R. P. (1993). The diagnosis of thoracic aortic dissection by noninvasive imaging procedures. New England Journal of Medicine, 328(1), 1-9. doi:10.1056/NEJM199301073280101
Olsson, C., Thelin, S., Ståhle, E., Ekbom, A., & Granath, F. (2006). Thoracic aortic aneurysm and dissection: Increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14 000 cases from 1987 to 2002. Circulation, 114(24), 2611-2618. doi:10.1161/CIRCULATIONAHA.106.630400
Pacini, D., Leone, A., Belotti, L. M. B., Fortuna, D., Gabbieri, D., Zussa, C., Contini, A., & Di Bartolomeo, R. (2013). Acute type A aortic dissection: Significance of multiorgan malperfusion. European Journal of Cardio-Thoracic Surgery, 43(4), 820-826. doi:10.1093/EJCTS/EZS500
Pape, L. A., Awais, M., Woznicki, E. M., Suzuki, T., Trimarchi, S., Evangelista, A., Myrmel, T., Larsen, M., Harris, K. M., Greason, K., et al. (2015). Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the international registry of acute aortic dissection. Journal of the American College of Cardiology, 66(4), 350-358. doi:10.1016/J.JACC.2015.05.029
Park, S. W., Hutchison, S., Mehta, R. H., Isselbacher, E. M., Cooper, J. V., Fang, J., Evangelista, A., Llovet, A., Nienaber, C. A., Suzuki, T., et al. (2004). Association of painless acute aortic dissection with increased mortality. In Mayo Clinic Proceedings, 79(10), 1252-1257. Elsevier. doi:10.4065/79.10.1252
Parvez, B., Sinha, D. J., Rawat, M., Pranshu, P., & Mehra, D. (2021). Morphological variations in mandibular anterior: Case studies. Annals of Dental Specialty, 9(4), 43-47.
Patel, P. D., & Arora, R. R. (2008). Pathophysiology, diagnosis, and management of aortic dissection. Therapeutic Advances in Cardiovascular Disease, 2(6), 439-468. doi:10.1177/1753944708090830
Ptaszek, L. M., Kim, K., Spooner, A. E., MacGillivray, T. E., Cambria, R. P., Lindsay, M. E., & Isselbacher, E. M. (2015). Marfan syndrome is associated with recurrent dissection of the dissected aorta. The Annals of Thoracic Surgery, 99(5), 1616-1623. doi:10.1016/J.ATHORACSUR.2014.12.066
Roberts, C. S., & Roberts, W. C. (1991). Dissection of the aorta associated with congenital malformation of the aortic valve. Journal of the American College of Cardiology, 17(3), 712-716. doi:10.1016/S0735-1097(10)80188-3
Sueyoshi, E., Nagayama, H., Hayashida, T., Sakamoto, I., & Uetani, M. (2013). Comparison of outcome in aortic dissection with single false lumen versus multiple false lumens: CT assessment. Radiology, 267(2), 368-375. doi:10.1148/RADIOL.12121274
Suhartati, T., Fatimah, N., Yandri, Y., Kurniawan, R., Bahri, S., & Hadi, S. (2021). The anticancer, antimalarial, and antibacterial activities of moracalkon a isolated from Artocarpus kemando Miq. Journal of Advanced Pharmacy Education and Research, 11(4), 105-110.
Suzuki, T., Distante, A., & Eagle, K. (2010). Biomarker-assisted diagnosis of acute aortic dissection: How far we have come and what to expect. Current Opinion in Cardiology, 25(6), 541-545. doi:10.1097/HCO.0B013E32833E6E13
Suzuki, T., Distante, A., Zizza, A., Trimarchi, S., Villani, M., Salerno Uriarte, J. A., De Luca Tupputi Schinosa, L., Renzulli, A., Sabino, F., Nowak, R., et al. (2009). Diagnosis of acute aortic dissection by D-dimer: The international registry of acute aortic dissection substudy on biomarkers (IRAD-Bio) experience. Circulation, 119(20), 2702-2707. doi:10.1161/CIRCULATIONAHA.108.833004
Suzuki, T., Katoh, H., Watanabe, M., Kurabayashi, M., Hiramori, K., Hori, S., Nobuyoshi, M., Tanaka, H., Kodama, K., Sato, H., et al. (1996). Novel biochemical diagnostic method for aortic dissection: Results of a prospective study using an immunoassay of smooth muscle myosin heavy chain. Circulation, 93(6), 1244-1249. doi:10.1161/01.CIR.93.6.1244
Trimarchi, S., Eagle, K. A., Nienaber, C. A., Pyeritz, R. E., Jonker, F. H., Suzuki, T., O'Gara, P. T., Hutchinson, S. J., Rampoldi, V., Grassi, V., et al. (2010). Importance of refractory pain and hypertension in acute type B aortic dissection: Insights from the international registry of acute aortic dissection (IRAD). Circulation, 122(13), 1283-1289. doi:10.1161/CIRCULATIONAHA.109.929422
Tsai, T. T., Evangelista, A., Nienaber, C. A., Trimarchi, S., Sechtem, U., Fattori, R., Myrmel, T., Pape, L., Cooper, J. V., Smith, D. E., et al. (2006). Long-term survival in patients presenting with type A acute aortic dissection: Insights from the international registry of acute aortic dissection (IRAD). Circulation, 114(1 Suppl), I350–I356. doi:10.1161/CIRCULATIONAHA.105.000497
Tsai, T. T., Nienaber, C. A., & Eagle, K. A. (2005). Acute aortic syndromes. Circulation, 112(24), 3802-3813. doi:10.1161/CIRCULATIONAHA.105.534198
von Kodolitsch, Y., Nienaber, C. A., Dieckmann, C., Schwartz, A. G., Hofmann, T., Brekenfeld, C., Nicolas, V., Berger, J., & Meinertz, T. (2004). Chest radiography for the diagnosis of acute aortic syndrome. The American Journal of Medicine, 116(2), 73-77. doi:10.1016/J.AMJMED.2003.08.030
von Kodolitsch, Y., Schwartz, A. G., & Nienaber, C. A. (2000). Clinical prediction of acute aortic dissection. Archives of Internal Medicine, 160(19), 2977-2982. doi:10.1001/ARCHINTE.160.19.2977
Wang, Y., Tan, X., Gao, H., Yuan, H., Hu, R., Jia, L., Zhu, J., Sun, L., Zhang, H., Huang, L., et al. (2018). Magnitude of soluble ST2 as a novel biomarker for acute aortic dissection. Circulation, 137(3), 259-269. doi:10.1161/CIRCULATIONAHA.117.030469
Williams, D. M., Lee, D. Y., Hamilton, B. H., Marx, M. V., Narasimham, D. L., Kazanjian, S. N., Prince, M. R., Andrews, J. C., Cho, K. J., & Deeb, G. M. (1997). The dissected aorta: Part III. Anatomy and radiologic diagnosis of branch-vessel compromise. Radiology, 203(1), 37-44. doi:10.1148/RADIOLOGY.203.1.9122414
Williams, D. M., LePage, M. A., & Lee, D. Y. (1997). The dissected aorta: Part I. Early anatomic changes in an in vitro model. Radiology, 203(1), 23-31. doi:10.1148/RADIOLOGY.203.1.9122399
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.