Malocclusion is described as an abnormality of the teeth or a misalignment of the dental arches that are outside of what is considered normal. Malocclusion is the third most prevalent illness in dental care, behind dental caries and periodontal disease. It has numerous effects on the patient’s physical and mental well-being. We aimed to review the literature looking for the etiology of malocclusion, risk factors, clinical presentation, diagnosis, and management of this disease. PubMed database was used for articles selection, gathered papers had undergone a thorough review. Malocclusion is a complex disease that has affected some of the population. Malocclusion is connected to both cosmetic and functional difficulties and can harm one's quality of life. Some of the etiologies are fortunately avoidable and should be addressed as soon as feasible. Multiple steps should be taken in assessing the current patient situation along with exploring the possible underlying cause. A well-tailored management plan should be developed according to the newest recommendation, available resources, and patient’s needs.
INTRODUCTION
Malocclusion is an improper or misalignment relationship between the teeth of the lower and upper dental arches, when the jaws close (Yamany, 2019; Asgari et al., 2020; Zedgenizova et al., 2021). Malocclusion is a common disease encountered in dental care, specifically, it is the third following periodontal disease and dental caries and hence ranks third among global public health dental disease priorities (Singh & Sharma, 2014; Kumar et al., 2021). Children with specific malocclusion characteristics tend to have greater issues with psychology and social relationships as they grow up, and their quality of life decreases as well (Yu et al., 2019). A cross-sectional study conducted in Abha, Saudi Arabia targeting teenagers found 1219 (61%) of the entire sample had a Class I molar relationship, whereas 326 (16.3%) and 154 (7.7%), respectively, had Class II and III molar relationships (Asiry & AlShahrani, 2019). This paper aimed to review the possible related etiologies to this disease, how to evaluate and manage it.
MATERIALS AND METHODS
PubMed database was used for the selection process of relevant articles, and the following keys used in the mesh ((“Malocclusion"[Mesh]) AND (“Evaluation"[Mesh] OR "Etiology"[Mesh] OR "Clinical signs"[Mesh] OR "Management"[Mesh])). The articles were chosen for inclusion based on one of the following criteria: Malocclusion or Malocclusion risk factors, etiology, assessment, treatment, or diagnosis. All other articles that did not match the requirements by not having any of the inclusion criterion results in their topic were excluded.
Review
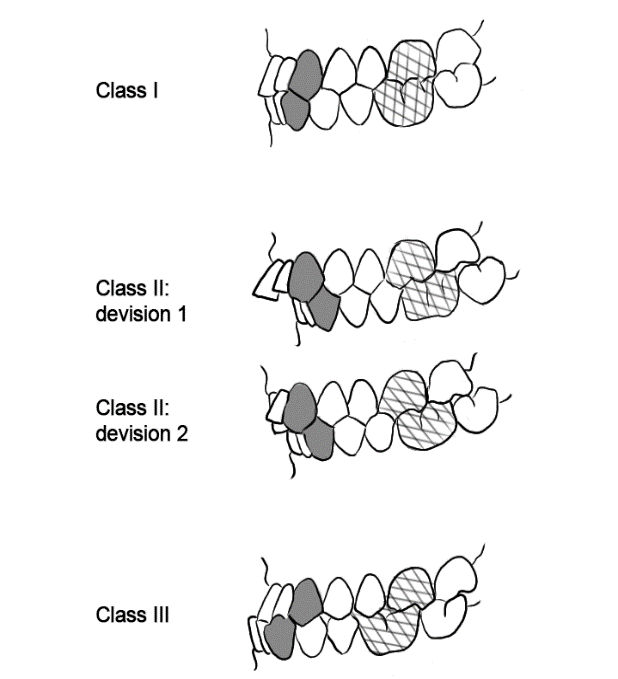
Classifying the malocclusion is a vital step to design the treatment plan and the measures to be taken. Angle’s classification is a famous one based on the maxillary first molar's relative location. The buccal groove of the mandibular first molar should coincide with the mesiobuccal cusp of the upper first molar. The teeth should all fit on a smooth occlusion line that runs through the central fossae of the posterior teeth and the cingulum of the incisors and canines in the upper arch and the buccal cusps of the posterior teeth and the incisal margins of the front teeth in the lower arch. Angle divided the malocclusions into three main classes: Class I, the molar connection of the occlusion is normal here, but the occlusion line is defective or as stated for the maxillary first molar, and the remaining teeth have issues such as crowding, spacing, over or under eruption, and so on. Class II The upper first molar's mesiobuccal cusp is not aligned with the lower first molar's mesiobuccal groove in this scenario. Rather, it is in front of it. The mesiobuccal cusp is usually seen between the first and second mandibular teeth. Class two has more two subcategories: Class II division 1, The anterior teeth are protruded, and the molar relationships are as previously described. Class II division 2, the central teeth are retroclined, and the lateral teeth overlap the central among the typical class II features. Lastly, in Class III, the upper molars are positioned behind the mesiobuccal groove, rather than in it. The maxillary first molar's mesiobuccal cusp is posterior to the mandibular first molar's mesiobuccal groove. Usually, the lower front teeth are more noticeable than the higher front teeth. The patient usually has a big mandible and a short maxillary bone in this scenario (Gravely & Johnson, 1974; Akbulut & Kılınç, 2019; Campbell & Goldstein, 2021). Figure 1 illustrates the different types of malocclusions.
|
|
|
Figure 1. Angle’s classification of the malocclusion |
Etiology
The etiologies behind the malocclusion safely can be categorized into congenital, acquired, and both. Where the combined form represents the majority of cases 64.3%, followed by acquired 29.7%, and finally the congenital representing only 4.5%. Therefore understanding the etiologies help in building better preventive and corrective management plans (Rapeepattana et al., 2019). Caries (22.5%), early loss of primary teeth (15.6%), and crowding, when the size of teeth is significantly disproportionate to the supportive bones, in the future permanent dentition (14.6%) were the top three orthodontic issues (Leighton, 1991; Rapeepattana et al., 2019; AlHumaidi et al., 2021). Losing teeth due to caries or trauma, which represent the first two causes, allows adhering teeth to migrate into the space. If the tooth is a deciduous molar, the successional tooth could be eliminated from the arch of teeth. Injury to deciduous incisors usually results in pulp death. Following the failure of the root to be absorbed, the successional incisor will be guided to an aberrant lingual position (Leighton, 1991; Alkilzy et al., 2007; Rapeepattana et al., 2019). Table 1 explores the detailed etiological causes (Rapeepattana et al., 2019).
Table 1. Possible etiological factors involved in malocclusions
|
Congenital |
Genetic: craniofacial development and tooth and occlusal development |
|
Gross defect of a rare type: facial cleft, micrognathia, absence of muscles, anodontia, and oligodontia, which are unknown in origin |
|
|
Acquired |
Postnatal injury: fracture of jaw and teeth, temporomandibular joint trauma |
|
Premature extraction of primary teeth, nature of food |
|
|
Habits affect lip action and mastication: nail-biting, tongue thrusting, posture, lip biting, lip sucking, thumb sucking, and others |
|
|
Local disease |
|
|
Nasopharyngeal disease and disturbed respiratory |
|
|
Gingiva and periodontal disease |
|
|
Tumors |
|
|
Caries |
|
|
Premature loss of primary teeth |
|
|
Disturbed in the sequence of eruption of permanent teeth |
|
|
Loss of permanent teeth |
|
|
Quality of tissue (forming, calcification) |
|
|
Unidentified |
Prenatal injury: mandible hypoplasia, Vogelgesicht, facial asymmetry |
|
Systemic diseases and endocrine disorder Others |
Clinical examination and evaluation
A thorough full dental examination backed with a detailed history to explore the possible pathophysiological course of the disease. The examination can be divided into two steps, the first involving the occlusal signs between the two jaws followed by measurement of space discrepancies within each jaw. The first step includes assessing the sagittal plane, transversal plane, and vertical plane for the lateral dental group. The sagittal plane is examined according to, previously mentioned, Angle’s classification. The transversal plane would be assessed for the narrowing in the two arches, maxillary and mandibular. If the narrowing is present in the former, it is a sign of posterior crossbite; and if the narrowing in the latter, it indicates scissor bite. The vertical plane is assessed for malocclusion space which may indicate a posterior open bite. Moreover, the sagittal plane is examined at the incisal level for positive and negative overjet, if the upper incisors were ahead or behind of the lower incisors, respectively. The second step looks for crowding and spacing, when the entire sum of slipped contacts for the incisor segment was at least 2 mm, it was considered crowding; when the total spacing for the incisor segment was at least 2 mm, it was considered spacing (Todor et al., 2019).
Management
Management of malocclusion varies in method and duration according to the type and the severity of each case. Mainly the method in use are conventional braces, Invisalign, and followed by retainer. Conventional braces are the mainstay device to use for its well-established results for more than a hundred years. By using brackets and a series of archwires, braces appliance is meant to shift teeth to their desired place. Edgewise brackets that have been pre-adjusted have a tip, torque, angulation, and in/out prescription incorporated into each one. The archwire is ligated into the bracket slots after the bands and brackets have been cemented and bonded in their optimal location. Invisalign was initially where meant to be used in mild to minor cases of crowding and spacing. Nevertheless, with the advanced technology in designing and material in use, Invisalign managed to break its way through more complicated cases with promising results and patients’ satisfaction. Invisalign's main advantage is esthetic and easy usage and maintenance (Nabhan et al., 2016; Khosravi et al., 2017; Ke et al., 2019). The term "orthodontic retention" refers to keeping teeth in their best cosmetic and functional positions following treatment. Two types of retainer are available, fixed and removable retainer; where their use varies according to the case. Some patients are advised to use them for the long term to preserve the obtained results. In such cases, a fixed retainer is preferred by orthodontists, which are attached to the lingual surfaces of the teeth and are both esthetic and simple to wear by patients for long-term usage (Kartal & Kaya, 2019).
CONCLUSION
Malocclusion is a multifactorial disease where many of the population succumbed to its consequences. Some of its highlighted etiologies are luckily preventable and should be taken off as early as possible. Malocclusion can have a detrimental influence on one's quality of life and is linked to aesthetic and functional issues. A variety of orthodontic equipment, both removable and fixed in nature, can be used to treat a malocclusion. Brackets and archwires are used in fixed orthodontic equipment to reposition teeth and treat the underlying malocclusion.
ACKNOWLEDGMENTS: The authors are greatfult to all support and guidance they got from Dr. Muqbil Saad Alqahtani.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Akbulut, A., & Kılınç, D. D. (2019). Evaluation of condyle position in patients with angle class I, II, and III malocclusion using cone-beam computed tomography panoramic reconstructions. Oral Radiology, 35(1), 43-50. doi:10.1007/s11282-018-0326-z
AlHumaidi, M. A., AlJahdali, S. L., AlGab, M. K. M., Alrizqi, A. A., AlShammeri, A. N., & AlQarni, A. A. (2021). Lasers related knowledge and practices of dentists in Riyadh City: A survey-based study. Annals of Dental Specialty, 9(3), 5-14.
Alkilzy, M., Shaaban, A., Altinawi, M., & Splieth, C. H. (2007). Epidemiology and aetiology of malocclusion among Syrian paediatric patients. European Journal of Paediatric Dentistry, 8(3), 131-135.
Asgari, I., Soltani, S., & Sadeghi, S. M. (2020). Effects of iron products on decay, Tooth microhardness, and dental discoloration: A systematic review. Archives of Pharmacy Practice, 11(1), 60-82.
Asiry, M. A., & AlShahrani, I. (2019). Prevalence of malocclusion among school children of Southern Saudi Arabia. Journal of Orthodontic Science, 8, 2. doi:10.4103/jos.JOS_83_18
Campbell, S., & Goldstein, G. (2021). Angle's classification–A prosthodontic consideration: Best evidence consensus statement. Journal of Prosthodontics, 30(S1), 67-71. doi:10.1111/jopr.13307
Gravely, J. F., & Johnson, D. B. (1974). Angle's classification of malocclusion: An assessment of reliability. British Journal of Orthodontics, 1(3), 79-86. doi:10.1179/bjo.1.3.79
Kartal, Y., & Kaya, B. (2019). Fixed orthodontic retainers: A review. Turkish Journal of Orthodontics, 32(2), 110-114. doi:10.5152/TurkJOrthod.2019.18080
Ke, Y., Zhu, Y., & Zhu, M. (2019). A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health, 19(1), 24. doi:10.1186/s12903-018-0695-z
Khosravi, R., Cohanim, B., Hujoel, P., Daher, S., Neal, M., Liu, W., & Huang, G. (2017). Management of overbite with the Invisalign appliance. American Journal of Orthodontics and Dentofacial Orthopedics, 151(4), 691-699. doi:10.1016/j.ajodo.2016.09.022
Kumar, P., Prasanth, T., Satisha, T. S., Gupta, N., & Manandhar, S. (2021). Photodynamic therapy - The light with therapeutic potential: A case series. Annals of Dental Specialty, 9(3), 72-76.
Leighton, B. C. (1991). Aetiology of malocclusion of the teeth. Archives of Disease in Childhood, 66(9), 1011-1012. doi:10.1136/adc.66.9.1011
Nabhan, A. F., Abbas, N. H., Fleming, P. S., Johal, A., & Sadek, M. M. (2016). Self‐ligating brackets versus conventional pre‐adjusted edgewise brackets for treating malocclusion. The Cochrane Database of Systematic Reviews, 2016(10). doi:10.1002/14651858.CD012407
Rapeepattana, S., Thearmontree, A., & Suntornlohanakul, S. (2019). Etiology of malocclusion and dominant orthodontic problems in mixed dentition: A cross-sectional study in a group of Thai children aged 8–9 years. Journal of International Society of Preventive & Community Dentistry, 9(4), 383-389. doi:10.4103/jispcd.JISPCD_120_19
Singh, V. P., & Sharma, A. (2014). Epidemiology of malocclusion and assessment of orthodontic treatment need for Nepalese children. International Scholarly Research Notices, 2014, 768357. doi:10.1155/2014/768357
Todor, B. I., Scrobota, I., Todor, L., Lucan, A. I., & Vaida, L. L. (2019). Environmental factors associated with malocclusion in children population from mining areas, western Romania. International Journal of Environmental Research and Public Health, 16(18), 3383. doi:10.3390/ijerph16183383
Yamany, I. A. (2019). The employment of CBCT in assessing bone loss around dental implants in patients receiving mandibular implant supported over dentures. International Journal of Pharmaceutical Research & Allied Sciences, 8(3), 9-16
Yu, X., Zhang, H., Sun, L., Pan, J., Liu, Y., & Chen, L. (2019). Prevalence of malocclusion and occlusal traits in the early mixed dentition in Shanghai, China. PeerJ, 7, e6630. doi:10.7717/peerj.6630
Zedgenizova, I., Ignatyeva, I., Zarubaeva, E., & Teplova, D. (2021). IT opportunities: Increasing the level of financial security in digital economy. Journal of Advanced Pharmacy Education and Research, 11(3), 157-161.
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.