Pediatric emergency services are thought to see a high incidence of medical errors (MEs). The emergency department (ED) is at the forefront of preventing medical errors, so the first step is to promote awareness of the issue and develop strategies to prevent errors and minimize harm when they occur. This study aims to summarize the current evidence regarding the prevalence, reporting, and outcome of medical errors in the pediatric emergency department to help improve safety and quality in pediatric emergencies. The previous studies were selected using the EBSCO information services and the PubMed database. All relevant publications were used for our estimation, including those related to medical errors in pediatric emergency departments. Other articles that are unrelated to this field were excluded. The data are extracted in a precise format that will be evaluated by the panel members. In conclusion, few studies have addressed medical errors in the pediatric emergency department. To report the budding number of ME proceedings, hospital management, and care providers can take several actions, such as increasing awareness of MEs in addition to the prominence of instance reporting, implementing working out and erudition workshops, and refining ME reportage.
INTRODUCTION
In healthcare, one of the main causes of morbidity and mortality is medical mistakes (Algahtani, 2020; Faller et al., 2020). Whether or not it is obvious or damaging to the patient, a medical mistake is an avoidable unfavorable outcome of medical treatment (Mangus & Mahajan, 2019). When providing medical care, problems like adverse drug events and improper transfusions, misdiagnosis, under and over-treatment, surgical injuries and wrong-site surgeries, suicides, injuries or deaths from restraints, falls, burns, pressure ulcers and patient identity confusion frequently come up. Pediatric patients receiving care in an acute or emergency setting may be particularly vulnerable to medical errors and abuse (Hofer et al., 2000).
Medical errors are common in the Emergency Department (ED), partly because the ED is frequently overburdened with patients who are severely ill or complicated. In a chaotic environment, emergency clinicians are frequently forced to make quick decisions, which increases the risk of error (Rinke et al., 2008). The clinician makes an early decision about a diagnosis and disregards other findings that could lead to a different conclusion. Among the most frequent medical errors are those related to drug administration (Al Meslamani et al., 2021). Children are predominantly vulnerable to medicinal errors due to age-related contraindications and the necessity for tailored dosage intention (Zed et al., 2013; Al-Hindi & Mojally, 2021).
Physician fatigue is linked to a lot of errors in pediatric emergency medicine (Mohammed-Jawad et al., 2020). Others mention the ED's frequent distractions. Some ED providers make cognitive errors often caused by poor communication. Staff in the emergency department must work together as a team (Kaufmann et al., 2012). ED providers must, without a doubt, communicate effectively with nurses and consultants. When this communication breaks down, it leads to a slew of mistakes (Alsalamah et al., 2021; Al-Mahroos et al., 2021). According to the Joint Commission, communication problems remain the 3rd greatest common source of custodian proceedings. Similarly, ED care providers must interconnect effectively through cases and their relatives to achieve a complete medical antiquity and collaborate on a treatment strategy (Ehsani et al., 2013).
Upholding a culture that works to distinguish security encounters and implement viable resolutions fairly rather than harboring a responsibility, embarrassment, and chastisement culture is part of the solution. Medical institutions must foster a culture of safety that values system development and sees medical mistakes as obstacles to overcome. All parts of the healthcare team must participate in making healthcare safer for patients and healthcare professionals (Brennan-Bourdon et al., 2020).
Study rationale
Of course, not all medical errors result in morbidity or mortality, but their prevalence makes it a problem worth addressing. The emergency department (ED) is on the front lines of preventing medical errors, so the first step is to advance the cognizance of the matter and develop strategies to prevent errors and minimize harm if they occur.
Study objective
The study aims to summarize current evidence regarding the prevalence, reporting, and outcome of medical errors in pediatric emergency departments to help improve safety and quality in pediatric emergencies.
MATERIALS AND METHODS
Study design
Integrative Literature Review (ILR).
Study duration
Data will be collected from 1–29 May 2022.
ILR is a technique for compiling previously published studies to synthesize suggestions on a subject; it is frequently utilized in the health disciplines to identify novelties and discover new approaches to health services, enabling the utilization of evidence-based health care, guaranteeing high-quality services, and enhancing patient welfare and safety. Six sequential stages are required to be followed: Explanation of the study issue; inclusion and exclusion criteria; sample definition; evaluation of included studies; findings interpretation; and presentation of the ILR synthesis.
The papers with the same goal as our study were reviewed in depth after searching and defining the sample. Following data collection, the information was grouped in a table, allowing the profile of the articles to be described, and the main points were highlighted.
Due to their reputation as reliable databases, PubMed and EBSCO Information Services were preferred as the exploration databases for the papers utilized in the study. One of the biggest online digital libraries, PubMed, was created by the National Center for Biotechnology Information (NCBI), a division of the National Library of Medicine of the United States. The article was created using subjects relating to medicinal errors in pediatric emergency rooms. The topics and summaries of the established papers were scrutinized.
The subjects were selected for addition founded on their applicability to the research, which must have at least one of the following subjects; medical errors, pediatric emergency, emergency department, reporting system, quality, and patient safety.
Exclusion criteria
All additional papers, recurring research, and reviews of research that do not possess one of these themes as their major end were disregarded.
Analysis of statistics
No software was used to examine the data. The data was extracted from a predefined form that also contained the research topic, author's title, goal, executive summary, findings, and outcomes. The outcomes of each affiliate were double-revised to ensure reasonableness and minimize inaccuracies.
Studies were double-reviewed throughout the article selection process to ensure that the research we included inside the study, and goal lines apply to the goal line of our study, and to avoid or decrease slips in the results.
RESULTS AND DISCUSSION
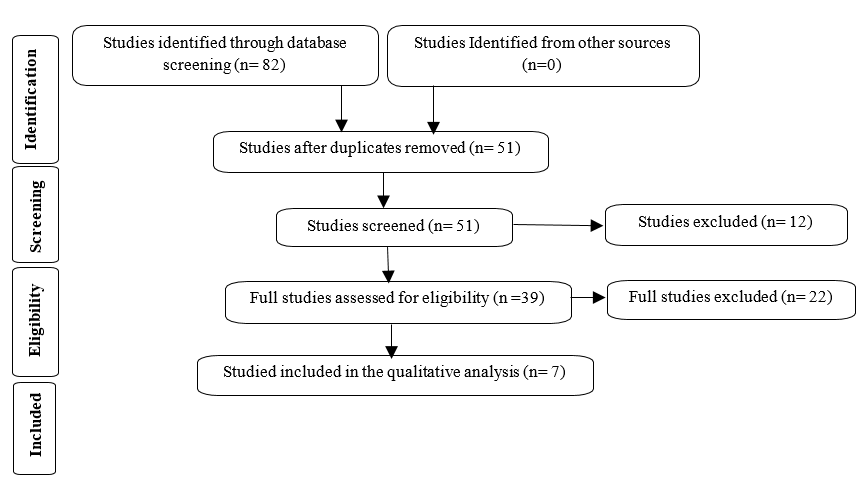
The assortment and documentation of the previous research are shown in (Figure 1). Eighty-two previous studies were found after searching the databases mentioned above, which were then used for title selection. Twelve of them were excluded due to the summary screening of 51 of them. The entire manuscripts of the outstanding 39 studies were examined. Seven papers were enlisted intended for the ultimate data abstraction after the complete manuscript amendment eliminated 22 research (Table 1).
Selbst and Krill (2020) reported 8 incidents of medical errors in the pediatric emergency room. Each case had a different teaching point to highlight this department's most frequent causes of medical errors.
Brennan-Bourdon et al. (2020) discussed medication errors in pediatric emergencies. Only 11.7% of all medications were deemed to be perfect prescription recommendations. In addition, the greatest communal MEs were the use of acronyms (50.9%) and incorrect pace of admin (11.4%).
Rinke et al. (2008) also discussed medication errors as 191 discrete diagrams and 377 in-house instructions each had a minimum of one error (12.5%, 10.8%, and 0.5%, respectively): instructions had an imprecise dose (1.1%), improper writing (10.8%), and improper writing with an inappropriate dose (0.5%). Out of 696 ambulatory prescriptions, (4.3%) had one error: (2.0%) had the wrong dose, and (2.3%) had been inscribed improperly. Pediatrics logged the greatest internal command wrong dosage error rate; postgraduate senior residents (3.5%), whereas the uppermost ambulatory medicine incorrect dose error frequency was logged by pediatrics postgraduate 2nd-year residents (ED) (9.1%)
De Muga et al. (2015) reported that the most frequent causes were human (70.7%), inadequate training (22.6%), and poor work circumstances (15.1%). Consequently, several actions were taken in these instances: operating specification, salbutamol unit dosages, and weight-standardized medication quantity tables for cardiopulmonary restoration.
Zed et al. (2013), in a systematic review, included 11 studies that reported medication-related ED visits or hospital admission in pediatric patients reported that hospice admittances and emergency department visits connected to medication varied from 0.16% to 4.3% and 0.5% to 3.3%, correspondingly. Of these, 20.3% to 66.7% were thought to be avoidable.
Kaufmann et al. (2012) found 32 original publications concerned with assessing methods for reducing error proportions in kid medicine orders. Using computer solutions for prescription orders with an integrated pediatric pharmacological database is strongly advised. The "pediatric crisis ruler" allows for precise measurement of the patient's weightiness in the prehospital situation. It also offers suggestions for age-suitable dosages and clearly shows the processes required to calculate the right dose.
The included studies had different study designs (Figure 1).
|
|
|
Figure 1. Prisma chart for data included in the study |
Table 1. Author, country, year of publication, methodology, and results
|
Author, Publishing Year |
Study Objective |
Methodology |
Study Outcome |
|
Selbst and Krill (2020) |
To summarize some cases of medical errors that occurred in the pediatric emergency department. |
A case series study |
To reduce medical mistakes, the study emphasizes the significance of maintaining excellent communication, paying attention to detail, listening carefully to patients and families, forming a broad differential, and avoiding premature closure before establishing a diagnosis. |
|
Brennan- Bourdon et al. (2020) |
In a public secondary-tertiary level hospital in Mexico, to define and analyze MEs during the prescription stage in pediatric critical care services. |
A cross-sectional investigation of all pediatric intensive care units at a public teaching hospital. Direct observation by a pharmacist served as the mistake detection technique, and MEs were categorized per the most recent categorization for medication errors. |
A total of 1252 possible MEs (72%) were found in 2347 drugs from 301 patients across all serious care services, and 379 of them were deemed clinically significant due to their potential damage. |
|
De Muga et al. (2015) |
A total of 1252 possible MEs (72%) were found in 2347 drugs from 301 patients across all critical care services, and 379 of them were deemed clinically significant due to their potential damage. |
A 2012 observational research that collected occurrences recorded between 2007 and 2011, which prospectively increased the volume of reports, examined their reasons, and enhanced customer input to the service, implemented a model update in May 2012. |
Only 19 incidences in the first model and 106 events in the second model were reported (5.6 times more). Medication events made up 57% of the reported incidents, followed by identification and procedures (26%). (7% ). |
|
Zed et al. (2013) |
To examine and summarize the most recent research on pediatric patients' medication-related ED and hospital admissions, including its occurrence, categorization, severity, preventability, and effect. |
The databases PubMed, Embase, and Web of Science were all thoroughly searched. Full reports of pediatric (under 18 years) patients who needed to go to the emergency room (ED) or be admitted to the hospital as a result of an adverse drug event (ADE) were included. |
On a range of 5.1% and 22.1% of the time, patients who visited the ED were hospitalized for stays ranging from 24 to 72 hours. Most ADEs were considered to be of moderate severity. Adverse drug responses, allergic reactions, overdoses, using medications without a prescription, prescribing the incorrect medicine, and giving a patient the wrong medication are some examples of ADEs. Breathing medications, antimicrobials, medicines for the central nervous system, analgesics, hormones, medicines for the heart, and vaccinations were common culprits. |
|
Kaufmann, et al. (2012) |
To assess the medicine ordering process and outline the possible solutions tested thus far for reducing mistake rates. |
Systematic literature review |
Interventions that increase prescribers' understanding of pediatric pharmacotherapy and tools that support the cognitive process of prescribing medicine can reduce error rates (calculators, computer programs, tables of doses by weight). They can also be reduced by organized communication, standardized, plainly labeled drug formulations, raising awareness of the issue of incorrect medication ordering, and monitoring prescription orders. |
|
Rinke et al. (2008) |
To assess the prevalence, source, and prescribing mistakes in ambulatory prescriptions and written in-house orders in a Pediatrics emergency room (PED). |
A 17-day backward chart review and a 6-month backward ambulatory prescription review for drugs with weight-based dosage in a PED. Prescriber identification number, method, weight-based target dose in milligrams per kilogram, frequency, appropriate dosing and medication allergies were all verified on orders and prescriptions. |
The greatest mistake rates for wrongly writing orders and prescriptions were seen in pediatrics ED attending doctors, at 25% and 9.7%, respectively. The most frequently used drugs in mistakes were opioids, analgesics, and antibiotics. |
|
Selbst et al. (1999) |
To begin looking at the drug mistakes that happen in a pediatric emergency room. These mistakes might result in considerable morbidity and mortality, as well as costly legal action. |
An analysis of all pharmaceutical and intravenous fluid mistakes found in a pediatric emergency department through event reports submitted over five years, as documented in retrospective charts. The patient outcomes were recorded and categorized using previously established criteria for clinical significance. |
Analysis was done on 33 event reports involving prescription or intravenous fluid mistakes. The evening and night shifts saw the majority of mistakes. 39 % of reported mistakes involved nurses, and 36 % involved both an emergency physician and a nurse. The most typical mistake was giving the wrong drug or the wrong dose. The family was not informed of the inaccuracy in one-third of the cases. Patients in 12% of cases needed extra care, and one patient had to be admitted to the hospital as a result of the mistake. Deaths weren't reported. |
Medical errors represent a serious public health problem and threaten patient safety. Due to the potential vulnerability of every patient, medical mistakes are expensive from a human, financial, and social perspective. Because emergency rooms can be so busy and chaotic, experts think that medical errors occur there even more frequently (La Pietra et al., 2005). Children, notably neonates and preterm infants treated in these settings are more prone to MEs because of the high-risk situations that surround critically sick children, particularly weight-based dosing errors and delayed medication administration (World Health Organization, 2016).
According to a study by Grasso et al., severe MEs have negative clinical outcomes and expose patients to difficulties in the form of high medical costs, lengthy hospital stays, and complications (Bates et al., 1999). Numerous studies have shown that higher mortality rates are related to MEs with high and high severity. Poor coordination and a lack of training programs to inform HCPs of the significance of reporting MEs once they occur make the issue worse. Additionally, most healthcare institutions don't have a grading system for identifying adverse events like MEs (AEs) (Harding & Petrick, 2008; Lisby et al., 2010).
In pediatric emergency medicine and office settings, physician burnout or fatigue is one of the most frequent causes of medical errors. According to the data, at least one out of every three physicians is currently burnt out. Patient satisfaction, care quality, physician alcohol, and drug abuse, and addiction correlate with physician burnout. Medical error rates are also directly correlated with burnout. Due to demanding schedules and "marathons" or multi-hour, back-to-back shifts, many medical professionals become exhausted. Due to symptoms like declining cognitive function, memory deficits, and impaired learning, a doctor is more likely to make a serious medical error the more exhausted they are (Rodziewicz et al., 2022).
Frequent interruptions and/or distractions frequently cause medical errors due to the hectic environment of emergency medicine clinics and office settings. For instance, a doctor might be attending to one patient when a more serious emergency case arrives. An even more instance is when a staff member needs to end a visit to speak with the medical provider about medication or surgery for another patient (World Health Organization, 2016).
It can be disastrous if there is poor communication between the staff, consultants, and patients/families. A pediatric patient may be seeing several different specialists. The patient and their family could miss important information if the specialists do not communicate with one another. This may result in serious medication issues, understanding which symptoms should prompt a return visit to the emergency room, following discharge instructions, and other crucial medical information (Ahmed et al., 2019). Selbst and Krill (2020) reported (Case 8) that the patient underwent left lower extremity amputation due to poor communication between an ED physician and nursing staff. It was discovered that the nursing staff's first triage notes described "+3 edema of the left leg and pedal pulses that couldn't be felt by touch.
No matter the situation, making quick decisions in an emergency environment can be challenging. Still, it can be especially challenging when a young patient's health, and sometimes even life, is at stake. When a doctor is fatigued or burned out, it is even harder for them to make quick decisions (Williams, 2007).
Tang and colleagues argue that proactive management processes must be in place to reduce MEs in healthcare facilities. Potential AEs can be minimized and prevented with the aid of a proactive risk management system, such as root-cause analysis. The root-cause analysis involves a system that can be used to spot underlying dangers that encourage patients, caregivers, and other stakeholders to make avoidable mistakes (Tang et al., 2007). Assistants and colleagues also encourage the use of computerized technology systems to enhance communication and reduce possible bias while decreasing human mistakes in prescription and drug errors. Information technology may also be utilized to synchronize data between departments, brought on by incorrect labeling, incorrect spelling, and sloppy handwriting.
By additional research, automation may help improve security, lower errors, and circumvent human limitations when providing healthcare (Stubbs et al., 2006).
A recent report on healthcare quality recommended an extensive approach to MEs in the Middle East. The authors also emphasized the importance of learning about and identifying MEs through optional and required reporting systems. Addressing significant AEs that routinely occur in healthcare activities would require adopting such an approach (Abduldaeem et al., 2016).
CONCLUSION
To report the budding number of ME proceedings, hospital management, and care providers can take several actions, such as raising awareness of MEs in addition to the prominence of instance reporting, implementing working out and erudition workshops, and refining ME reportage. Additional successful ME preventive tactics include regular assessments of MEs and their effects on care delivery, the promotion of training initiatives, and stringent quality control standards for all HCPs.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Abduldaeem, H., Masters, K., Patel, N., & Donyai, P. (2016). A direct observation study of medication administration errors in a mental health inpatient setting. IJPP, 24(Supp. 1), 4-29.
Ahmed, Z., Saada, M., Jones, A. M., & Al-Hamid, A. M. (2019). Medical errors: Healthcare professionals’ perspective at a tertiary hospital in Kuwait. PloS One, 14(5), e0217023. doi:10.1371/journal.pone.0217023
Al Meslamani, A. Z., Abdel-Qader, D. H., Albassam, A., Ismael, N. S., Asma'A, E. S., Lewis, P., Hamadi, S., Al Jomaa, E., & Al Mazrouei, N. (2021). Pharmacy students' knowledge and attitude of prescribing errors. Journal of Advanced Pharmacy Education & Research, 11(1), 106-113.
Algahtani, F. D. (2020). Healthy Lifestyle among Ha'il University Students, Saudi Arabia. International Journal of Pharmaceutical Research and Allied Sciences, 9(1), 160-167.
Al-Hindi, Y., & Mojally, M. (2021). MyDispense impact in compensating summer field training course during COVID-19 pandemic. Journal of Advanced Pharmacy Education and Research, 11(1), 35-38.
Al-Mahroos, M. I. A., Al-Tamimi, D. J. J., Al-Tamimi, Z. J. J., & Ibraheem, J. J. (2021). Clinical pharmacokinetics and bioavailability study between generic and branded fluconazole capsules. Journal of Advanced Pharmacy Education and Research, 11(1), 161-169.
Alsalamah, M., Alwallan, N. S., Alshahrani, S. M., Al-Khateeb, B. F., Aldahash, R., Angawi, K., Toivola, P., & El-Metwally, A., (2021). Predictors of prolonged adult hospitalization in the tertiary care hospital emergency department of Saudi Arabia. Journal of Advanced Pharmacy Education & Research, 11(3), 95-100.
Bates, D. W., Miller, E. B., Cullen, D. J., Burdick, L., Williams, L., Laird, N., Petersen, L. A., Small, S. D., Sweitzer, B. J., Vander Vliet, M., et al. (1999). Patient risk factors for adverse drug events in hospitalized patients. ADE prevention study group. Archives of Internal Medicine, 159(21), 2553-2560.
Brennan-Bourdon, L. M., Vázquez-Alvarez, A. O., Gallegos-Llamas, J., Koninckx-Cañada, M., Marco-Garbayo, J. L., & Huerta-Olvera, S. G. (2020). A study of medication errors during the prescription stage in the pediatric critical care services of a secondary-tertiary level public hospital. BMC Pediatrics, 20(1), 549. doi:10.1186/s12887-020-02442-w
de Muga, M. V., Llop, A. S., Escudero, E. R., Contreras, M. J., & Cubells, C. L. (2015). Impact on the improvement of paediatric emergency services using a standardized model for the declaration and analysis of incidents. Anales de Pediatría (English Edition), 83(4), 248-256.
Ehsani, S. R., Cheraghi, M. A., Nejati, A., Salari, A., Esmaeilpoor, A. H., & Nejad, E. M. (2013). Medication errors of nurses in the emergency department. Journal of Medical Ethics and History of Medicine, 6, 11.
Faller, E. M., Hernandez, M. T., Hernandez, A. M., & Gabriel, J. R. S. (2020). Emerging roles of pharmacist in global health: An exploratory study on their knowledge, perception and competency. Archives of Pharmacy Practice, 11(1).
Harding, L., & Petrick, T. (2008). Nursing student medication errors: A retrospective review. The Journal of Nursing Education, 47(1), 43-47.
Hofer, T. P., Kerr, E. A., & Hayward, R. A. (2000). What is an error? Effective Clinical Practice: ECP, 3(6), 261-269.
Kaufmann, J., Laschat, M., & Wappler, F. (2012). Medication errors in pediatric emergencies: A systematic analysis. Deutsches Arzteblatt International, 109(38), 609-616. doi:10.3238/arztebl.2012.0609
La Pietra, L., Calligaris, L., Molendini, L., Quattrin, R., & Brusaferro, S. (2005). Medical errors and clinical risk management: State of the art. Acta Otorhinolaryngologica Italica, 25(6), 339-346.
Lisby, M., Nielsen, L. P., Brock, B., & Mainz, J. (2010). How are medication errors defined? A systematic literature review of definitions and characteristics. International Journal for Quality in Health Care, 22(6), 507-518. doi:10.1093/intqhc/mzq059
Mangus, C. W., & Mahajan, P. (2019). Common medical errors in pediatric emergency medicine. Clinical Pediatric Emergency Medicine, 20(3), 100714.
Mohammed-Jawad, N. K., Abdulrahman, N. M., Emad, A., & Jumaa, S. (2020). Assessment of dosing errors in pediatric patients prescriptions in Basra city. Archives of Pharmacy Practice, 11(1), 73-76.
Rinke, M. L., Moon, M., Clark, J. S., Mudd, S., & Miller, M. R. (2008). Prescribing errors in a pediatric emergency department. Pediatric Emergency Care, 24(1), 1-8. doi:10.1097/pec.0b013e31815f6f6c
Rodziewicz, T. L., Houseman, B., & Hipskind, J. E. (2022). Medical error reduction and prevention. StatPearls [Internet].
Selbst, S. M., Fein, J. A., Osterhoudt, K., & Ho, W. (1999). Medication errors in a pediatric emergency department. Pediatric Emergency Care, 15(1), 1-4. doi:10.1097/00006565-199902000-00001
Selbst, S., & Krill, K. (2020). Medical errors in the pediatric emergency department: Don't make these mistakes! Contemporary Pediatrics, 37, 24-26.
Stubbs, J., Haw, C., & Taylor, D. (2006). Prescription errors in psychiatry–A multi-centre study. Journal of Psychopharmacology, 20(4), 553-561. doi:10.1177/0269881106059808
Tang, F. I., Sheu, S. J., Yu, S., Wei, I. L., & Chen, C. H. (2007). Nurses relate the contributing factors involved in medication errors. Journal of Clinical Nursing, 16(3), 447-457.
Williams, D. J. (2007). Medication errors. Journal-Royal College of Physicians of Edinburgh, 37(4), 343.
World Health Organization. Medication errors: Technical series on safer primary care. Geneva: World Health Organization; 2016. License: CC BY-NC-SA 3.0 IGO.
Zed, P. J., Haughn, C., Black, K. J., Fitzpatrick, E. A., Ackroyd-Stolarz, S., Murphy, N. G., MacKinnon, N. J., Curran, J. A., & Sinclair, D. (2013). Medication-related emergency department visits and hospital admissions in pediatric patients: A qualitative systematic review. The Journal of Pediatrics, 163(2), 477-483. doi:10.1016/j.jpeds.2013.01.042
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.