Cleft lip occurs when the frontonasal and maxillary processes fail to the lip. Moreover, cleft palate results when the fusion of the palatal shelves of the maxillary fail to complete, both soft and hard palate can be affected with or without cleft lip. In Saudi Arabia, the prevalence of cleft lip and palate (CLP) is at 0.65 per 1000 live births, with boys accounting for 63.7 percent and girls for 36.6 percent. We aimed to review the literature reviewing etiology of cleft lip and/or palate, clinical presentation, diagnosis, and management of this disease. PubMed database was used and the following keys used in the mesh ((“Cleft lip"[Mesh] OR "Cleft palate"[Mesh] OR "CLP"[Mesh]) AND (“Etiology "[Mesh] OR " Clinical Presentation"[Mesh] OR "Management"[Mesh])). CLP are congenital abnormalities that impact a variety of structures and functions, including appearance, speech difficulties, psychology, and eating and nutrition. Extensive dental treatment and a multidisciplinary approach to this condition are required at the appropriate time and age.
INTRODUCTION
Cleft lip, palate, or both (CLP) is a condition where there is a significant malformation of the one of aforementioned structures. The cleft lip arises when the frontonasal and maxillary processes fail to fuse to a different extent through the lip. Cleft palate occurs when the fusion of the palatal shelves of the maxillary fails to complete, both soft and hard palate can be affected (Vyas et al., 2020). The prevalence of cleft lip and palate in a recent study in Saudi Arabia found that it is 0.65 per 1000 live births (Alyami et al., 2020; Al-Turck et al., 2021). Variation between males and females ratio was evident in two more studies, where the males reported a percentage of (63.7%) and females’ of (36.6%) (Al-Balkhi, 2008; Sabbagh et al., 2012). Different perceptions and interpretations of this anomaly are scattered across the cultures based on folklore and religious beliefs, which include superpower, witchcraft, reincarnation, and the evil eye (Mednick et al., 2013). Hence, those misperceptions should be clarified for society in general and the family in particular.
MATERIALS AND METHODS
For selecting processing relevant articles, PubMed database was used and the following keys used in the mesh ((“Cleft lip"[Mesh] OR "Cleft palate"[Mesh] OR "CLP"[Mesh]) AND (“Etiology "[Mesh] OR " Clinical Presentation"[Mesh] OR "Management"[Mesh])). The articles were chosen for inclusion according to one of the following criteria: etiology, clinical presentation, and management of cleft lip or cleft palate. All other articles that matched the requirements by having none of the inclusion criteria findings in their topic were excluded.
RESULTS AND DISCUSSION
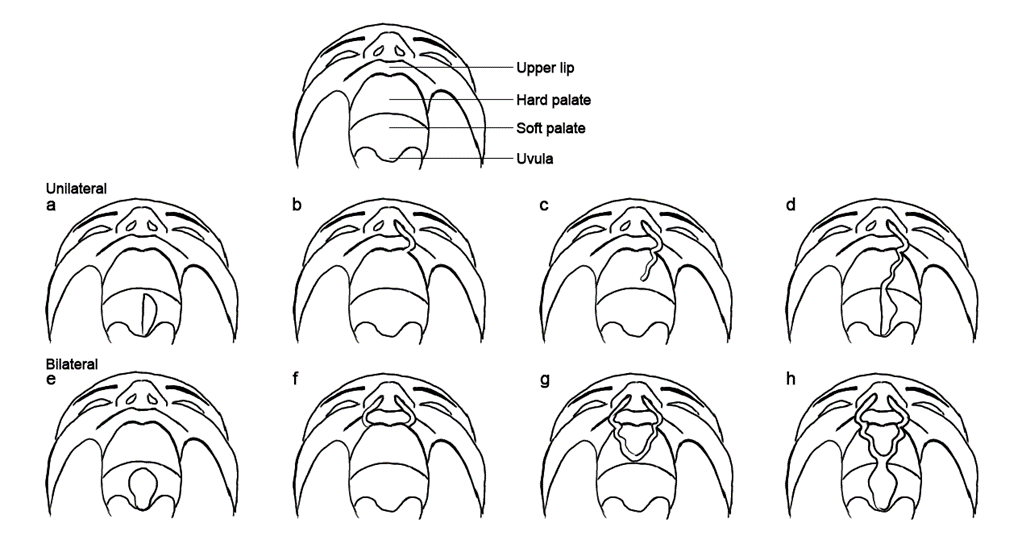
Different classifications have been proposed throughout the past century where some relied on etiology, pathogenesis, or affected anatomical parts. For a better understanding of the severity, thence better management, the combination of all the proposed classification is recommended. Figure 1 describes all the possibilities of cleft lip and/or palate (Jagomägi, 2011).
|
|
|
Figure 1. Types of clefts. a. unilateral cleft of the soft palate; b. unilateral cleft lip; c, d unilateral cleft lip, and palate; e. bilateral cleft of the soft palate; f. bilateral cleft lip; g,h. bilateral cleft lip and palate. |
Etiology
The factors that contribute to cleft malformation are complex and mostly interconnected, broadly can be categorized into genetics and non-genetics factors. Exposure to a teratogen during pregnancy showed significant evidence in studies. Smoking for instance is a weak but evident factor, 1.3 to 1.5 relative risk associated with CLP. Moreover, if this factor is presented alongside relevant genotypes, this risk can rise to 7.16 times (Kohli & Kohli, 2012; Elmorsy et al., 2021). Alcohol consumption during pregnancy also showed a dose-dependent effect ranging from 1.5 to 4.7, regardless of the genetic predisposition (Kohli & Kohli, 2012). Other contributing factors include maternal chronic diseases, increase maternal and paternal age, and retinoid exposure (Lorente & Miller, 1978; Bille et al., 2005; De Sousa et al., 2009).
Genetics plays a major role in CLP, in that is observable in comparing monozygotic against dizygotic twins. Genetic causes can be further subclassified as syndromic and non-syndromic. For the former refer to Table 1. On the other hand, non-syndromic causes comprise up to 70% of overall cases of CLP, Table 2 states thee possible mutations related to CLP (Lorente & Miller, 1978; Bille et al., 2005; Jagomägi, 2011).
Table 1. Syndromic form of cleft lip and palate
|
Waardenburg syndrome, type II A |
|
Di George syndrome |
|
Treacher - Collins mandibulofacialdysostosis |
|
Van der woude syndrome |
|
CLP-Ectodermal dysplasia syndrome |
|
Ectrodactyly, ectodermal dysplasia orofacial cleft syndrome |
|
Zollinger syndrome-3 |
|
Diastrophic dysplasia |
|
Gorlin syndrome (Basal cell nevus syndrome) |
Table 2. Genetic mutations related to cleft lip and palate
|
Name of gene |
Symbol |
Chromosome location |
|
Transforming growth factor-alpha |
TGFA |
2p13 |
|
Transforming growth factor - 133 |
TGF 133 |
14q24 |
|
Methylene tetra - hydro folate reductase |
MTHF3 |
1p36,3 |
|
Blood clotting factor XIII gene |
ET1 |
6p24 |
|
Endothelin - 1 gene |
ET1 |
6p24 |
|
Proto-oncogene BCL3 |
BCL3 |
19q13,2 |
|
Retinoic acid receptor alpha gene |
RARA |
17(t15/17) |
Clinical presentation
The detection of the problem is usually early detected but the treatment, unfortunately, is not always readily available due to different causes according to the financial and cultural causes. The most part affected by CLP is the dentation processes. Where various problems erupt due to the malformed maxillary plate. Microdontia, small teeth, is commonly seen in the lateral incisors, where they become peg-shaped (Kadam et al., 2013). Taurodontism, tooth’s body is irregularly enlarged and taken from the root space, this condition is typically associated with syndromic causes. Due to the lack of space, the ectopic eruption is seen in lateral incisors and canines as they tend to be placed on the palate instead (Jamal et al., 2010; Pradhan et al., 2020). Other non-dental issues are also encountered, the feeding problem is a crucial and complicated one. A deformed palate makes it hard for the infant to attach and suckle from the nipple normally, therefore proper education for the mother and training with the specialized nipple to ensure the wellbeing of the infant’s nutrition (Hiremath et al., 2016). Ear infection is also common with CLP patients due to the deformity of the Eustachian tube, recurrent otitis media is commonly present and require immediate intervention to avoid permanent hearing problems (Wang et al., 2019; Kryukova et al., 2021).
Management
The definitive management of CLP is a surgical one, nevertheless, a multidisciplinary team is needed to ensure the best outcome and rehabilitation of the patient. As previously mentioned, ENT doctors should be present for the possibility of hearing problems, speech therapist also might be needed before and after the correction. In the presence of a cleft in the lip, taping the lips is the initial step to take before the permanent closure of the palate. The technique that is widely used is naso-alveolar molding (NAM), which showed decent results in terms of cosmesis and function. NAM prosthesis requires 24 hours placement and highly motivated and compliant parents, with adjustment every week or every other week (Worley et al., 2018). Three techniques are commonly used in repairing the palate; straight-line repair with intravelar veloplasty or two-flap palatoplasty, Veau-Wardill-Kilner V-Y pushback, and Furlow double Z-plasty.
Two-flap palatoplasty or straight-line repair with intravelar veloplasty
Mucoperiosteal flaps on each side of the cleft are elevated using this method. From the maxillary alveolus to the soft palate, nasal and oral mucosal flaps are raised anteriorly. Over the soft palate, the flap's medial mucosal attachments are solely left intact. After that, the flaps are laminated and turned medially. The muscular attachments are raised from the hard palate and placed in the midline more posteriorly at the soft palate to restore the levator muscle sling. A short palate is not lengthened by this approach (Fakhim et al., 2020; Pradhan et al., 2020).
Furlow double Z-plasty
Mucosal flaps in a second layer to re-create the uvula, the transposition of soft palatal muscle, or Z-plasty flaps in one layer to re-create the levator sling, are used in the Furlow palatoplasty. The Z-plasty procedure allows the palate to be stretched. For the closure of the hard palate cleft, straight-line mucoperiosteal flaps are lifted (Agrawal, 2009; Fakhim et al., 2020).
Veau-wardill-kilner V-Y pushback
Bilateral mucoperiosteal flaps elevation, which involves oral mucosa in an anterior to posterior orientation is used in this method. The flaps' posterior attachments are still intact. Then, mucoperiosteal flaps are pushed back and repositioned at the midline, which as a result, makes palatal lengthening possible (Agrawal, 2009).
CONCLUSION
Cleft lip and/or palate is a fairly preventable malformation if the triggering environmental factors were avoided during the pregnancy. Educating future moms, as well as fathers, might result in the reduction of the incidence rate. CLP are congenital abnormalities that impact a variety of structures and functions, including appearance, speech difficulties, psychology, and eating and nutrition. To attain functional and aesthetic well-being, patients with CLP deformity must be treated at the appropriate time and the appropriate age. Extensive dental treatment and a multidisciplinary approach to this condition are required, to ensure the overall life quality enhancement.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Agrawal, K. (2009). Cleft palate repair and variations. Indian Journal of Plastic Surgery, 42(S 01), S102-S109. doi:10.4103/0970-0358.57197
Al-Balkhi, K. M. (2008). The distribution and classification of clefts in patients attending a cleft lip and palate clinic in Riyadh, Saudi Arabia. Saudi Medical Journal, 29(5), 739-742.
Alyami, B., Ali-Hassan, M., Braimah, R., Al-Mahri, M., Alyami, F., & Alharieth, S. (2020). Prevalence and clinical case series of syndromic and nonsyndromic cleft lip and palate in a Saudi Arabian neonatal population. The Cleft Palate-Craniofacial Journal, 57(11), 1259-1265. doi:10.1177/1055665620929247
Al-Turck, K., Alsaeri, N., Alanazi, R., Alajaji, R., Alsulaiman, S., Al-Jehani, N., & Alodaini, F. (2021). Self- reported oral care and oral health among women during pregnancy, Riyadh, Saudi Arabia. Annals of Dental Specialty, 9(2), 79-85.
Bille, C., Skytthe, A., Vach, W., Knudsen, L. B., Andersen, A. M. N., Murray, J. C., & Christensen, K. (2005). Parent’s age and the risk of oral clefts. Epidemiology (Cambridge, Mass.), 16(3), 311. doi:10.1097/01.ede.0000158745.84019.c2
De Sousa, A., Devare, S., & Ghanshani, J. (2009). Psychological issues in cleft lip and cleft palate. Journal of Indian Association of Pediatric Surgeons, 14(2), 55-58. doi:10.4103/0971-9261.55152
Elmorsy, A. K., Hafez, A. M., Fouda, A. M., & El-Bialy, A. A. (2021). Success rate of miniscrew anchorage for miniscrew anchored maxillary protraction. Annals of Dental Specialty, 9(2), 62-65.
Fakhim, S. A., Nouri-Vaskeh, M., Amiri, F., & Shahidi, N. (2020). Comparison of two-flap palatoplasty plus intravelar veloplasty technique with and without double-layer Z-plasty on the soft palate length in children with cleft palate. Oral and Maxillofacial Surgery, 24(4), 495-499. doi:10.1007/s10006-020-00884-1
Hiremath, V. S., Lingegowda, A. B., Rayannavar, S., & Kumari, N. (2016). A innovative technique-modified feeding bottle for a cleft palate infant. Journal of Clinical and Diagnostic Research: JCDR, 10(4), ZM01. doi:10.7860/JCDR/2016/15840.7526
Jagomägi, T. (2011). A study of the genetic etiology of nonsyndromic cleft lip and palate (Doctoral dissertation, Tartu University).
Jamal, G. A. A., Hazza'a, A. M., & Rawashdeh, M. A. A. (2010). Prevalence of dental anomalies in a population of cleft lip and palate patients. The Cleft Palate-Craniofacial Journal, 47(4), 413-420. doi:10.1597/08-275.1
Kadam, M., Kadam, D., Bhandary, S., & Hukkeri, R. Y. (2013). Natal and neonatal teeth among cleft lip and palate infants. National Journal of Maxillofacial Surgery, 4(1), 73. doi:10.4103/0975-5950.117883
Kohli, S. S., & Kohli, V. S. (2012). A comprehensive review of the genetic basis of cleft lip and palate. Journal of Oral and Maxillofacial Pathology: JOMFP, 16(1), 64. doi:10.4103/0973-029X.92976
Kryukova, E. M., Khetagurova, V. S., Ilyin, V. A., Chizhikova, V. V., & Kosoplechev, A. V. (2021). Forming students’ environmental culture: Modern educational approaches and technologies. Journal of Advanced Pharmacy Education and Research, 11(2), 113-118.
Lorente, C. A., & Miller, S. A. (1978). Vitamin A induction of cleft palate. The Cleft Palate Journal, 15(4), 378-385.
Mednick, L., Snyder, J., Schook, C., Blood, E. A., Brown, S. E., & Weatherley-White, R. C. A. (2013). Causal attributions of cleft lip and palate across cultures. The Cleft Palate-Craniofacial Journal, 50(6), 655-661. doi:10.1597/11-300R1
Pradhan, L., Shakya, P., Thapa, S., Nakarmi, K. K., Maharjan, A., Sagtani, R. A., & Rai, S. M. (2020). Prevalence of dental anomalies in the patient with cleft lip and palate visiting a tertiary care hospital. JNMA: Journal of the Nepal Medical Association, 58(228), 591-596. doi:10.31729/jnma.5149
Sabbagh, H. J., Mossey, P. A., & Innes, N. P. (2012). Prevalence of orofacial clefts in Saudi Arabia and neighboring countries: A systematic review. The Saudi Dental Journal, 24(1), 3-10. doi: 10.1016/j.sdentj.2011.11.001
Vyas, T., Gupta, P., Kumar, S., Gupta, R., Gupta, T., & Singh, H. P. (2020). Cleft of lip and palate: A review. Journal of Family Medicine and Primary Care, 9(6), 2621. doi:10.4103/jfmpc.jfmpc_472_20
Wang, C., Chen, R. J., & Zhou, Z. (2019). Characteristics of secretory otitis media in children with cleft palate and timing of intervention of tympanic membrane. Lin Chuang er bi yan hou tou Jing wai ke za zhi= Journal of Clinical Otorhinolaryngology, Head, and Neck Surgery, 33(7), 647-650. doi:10.13201/j.issn.1001-1781.2019.07.017
Worley, M. L., Patel, K. G., & Kilpatrick, L. A. (2018). Cleft lip and palate. Clinics in Perinatology, 45(4), 661-678. doi:10.1016/j.clp.2018.07.006
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.