Varus deformities of the lower limbs are common problems in both children (Blount disease), and the older age group. The classification and management is a great challenge requiring a multidisciplinary approach to prevent a recurrence. In addition, the associated morbidities need earlier detection and management. The current review highlighted the etiology, epidemiology, diagnosis, treatment, prognosis, and recurrence. Importantly, the review assessed the associated comorbidities that if not corrected might negatively affect the prognosis and endanger the patient's life. We searched the PubMed, Cochrane Library, and Google Scholar for recent trends in varus deformities; in addition, we searched the grey literature and screened the references of the included studies. The keywords " Varus deformities", "Blount disease", "rickets", "vitamin D deficiency", were used with protean "AND and OR". We identified 245 articles, of them eight full text were screened, and only three evaluated the association of Blount disease and vitamin D deficiency and were eligible for meta-analysis., other studies were included in a narrative review. The studies pooled in the meta-analysis included 1924 patients and 1661 events. No association was evident between vitamin D deficiency and BD (odds ratio, 4.13, 95% CI, 0.45-38.10, P-value, 0.21). However, the small number of the study included and considerable heterogeneity limited our results (I2 =93%, Chi-square, 28.79, and df =2). Further studies evaluating this important topic are recommended.
INTRODUCTION
Tibial deformities are common among children; they are either congenital or acquired. The management is faced with problems, obstacles, and complications (Tsibidakis et al., 2014). Taylor Spatial Frame has shown success among children with morbid obesity with minimal complications (Li et al., 2013). Fixation methods and osteotomy are effective; other surgical management includes lateral hemiepiphisyodesis and physeal bar resection. However, uniform weight distribution across the knee joint is vital (Vukašinović et al., 2013; Huang et al., 2014). Tibia vara (Blount's disease) is the most common cause of genu varum deformity among adolescents and children worldwide, the uneven stress distribution on foot bones and changes in loading of knee menisci, tibial articular cartilage, and subchondral bone was documented (Özkan et al., 2013). Obesity is a common risk factor for both tibia vara and slipped upper femoral epiphysis. Besides, the later deformities were found to co-exist (Sanghrajka et al., 2012; Jamil et al., 2015; Abdulsahib & Abood, 2021). Blount's disease (BD) is essentially multifactorial and the association with hypertension, vitamin D deficiency, morbid obesity, and rheumatic disorders was observed (Pereira‐Santos et al., 2015; Taussig et al., 2016; Rasheed et al., 2020). A multidisciplinary approach is needed to avoid treatment failure and recurrence. Thus, this review assessed investigated the association of vitamin D deficiency, slipped upper femoral epiphysis, obesity, hypertension, and BD.
Etiology
The etiology is multifactorial with genetic susceptibility and mechanical overload leading to osteochondrosis in the proximal tibial epiphysis and physis and ending in physical bars. Blacks and Hispanic obese males being the most affected (DMTS & De Leucio, 2020).
Epidemiology
There are two types, childhood that affected the age group 2-5 years and usually bilateral and more severe and a less severe unilateral adolescent variant (>10 years). With an intermediate type in-between. Black obese children are more affected in the Americas and Caribbean. Besides, the disease is more severe. However, these associations are not observed in other parts of the World (Janoyer, 2019; Abdul, 2021).
Diagnosis
Clinically the disease presented by bowing of tibia, limb shortening, and osteoarthritis of the knee joint.
X-ray: is the mainstay of diagnosis, Langenskiold classification is widely used with minimal inter-observer and intra-observer bias. The classification is based on epiphyseal depression and fragmentation at the proximal medial tibia. Six grades ranging from Medio-distal beaking of the upper proximal tibial metaphysis (stage 1) to closure with bony bridge (Langenskiold, 1952; Khanfour, 2012). Long-leg is needed (from hip to ankle bilaterally). Drennan angle (Metaphyseal-diaphyseal Angle) is a perpendicular line drawn from metaphyseal beaks along the tibial axis. An angle of less than 10° resolve in 95% of patients and close observation is needed for 11-16° (Park et al., 2019; DMTS & De Leucio, 2020). A magnetic resonance staging is also present. However, X-ray staging is widely used. Importantly, staging is only needed for the infantile type of BD.
Magnetic resonance imaging
Although the main pathology is the enlargement of medial menisci and mid-coronal thickness of the medial tibial epiphyseal cartilage. However, medial femoral epiphyseal cartilage may show increased signals in half of the patients. MRI is more accurate than a radiograph (detects the early cartilaginous changes) helps to delineate the extent of the disease in the lateral knee and other knee compartments (Ho-Fung et al., 2013).
Treatment
Follow-up is vital as spontaneous regression is observed in the infantile variant. The treatment is a complex surgery, so a thorough evaluation and planning for all deformities are needed. The severity and maturity of the patients are the two major determinants of the intervention. The goal of the treatment is to correct the three-dimensional deformity with minimal recurrence. Immature patients with moderate deformities are better treated with guided growth, while osteotomy or physeal distraction are good choices for severely affected patients who are more mature (de Pablos et al., 2018). Brace use is controversial, it might be helpful in non-obese children before 3 years of age, an osteotomy is needed before age four (Sabharwal & Sabharwal, 2017).
Graded growth
A minimum of four years of growth is needed, the treatment is based on the principle of compression inhibits longitudinal growth. Tension band plating, pinning, and Hemiepiphysiodesis of the lateral epiphysis with staples are used.
Prognosis
The prognosis is good in the infantile form, early detection and proper treatment are vital to prevent progression, recurrence, and complications.
A multidisciplinary approach for effective care
A collaborative teamwork is vital including a pediatric orthopedic Surgeon, Physical medicine and rehabilitation professionals for early rehabilitation, Orthotists if a brace is needed, and metabolic physician for the management of the associated metabolic disorders (DMTS & De Leucio, 2020).
Recurrence
A high recurrence rate was observed among patients with gross deformity with delayed presentation, and medial metaphyseal Slope (Laoharojanaphand et al., 2019), while the relationship with demographic factors including age is controversial (Chotigavanichaya et al., 2002; LaMont et al., 2019).
The importance of blount's disease and its confusing tail with rickets
Blount's disease is increasingly diagnosed due to the global rise of obesity among children, BD is a rickets mimicker, if not correctly diagnosed and managed promptly, and lethal complications might develop including deformities of the distal femur, knee, and tibia, in addition to short stature and premature osteoarthritis (Bhattacharjee et al., 2016; Kohnen et al., 2021). Table 1 illustrates a comparison between Blount,s disease and rickets.
Table 1. Blount's Disease versus Rickets
|
Character |
Blount's disease |
Rickets |
|
Cupping, fraying, and splaying of metaphyses |
Absent |
Present |
|
Deformity |
Proximal tibial deformity with medial beaking |
Diffuse bowing throughout the bone |
|
Obesity, African ethnicity, female sex, early walking factors |
Associated |
Not necessarily |
|
Involvement of upper limbs and enlargement of the costochondral junction |
Not present |
May be present |
|
Vitamin D deficiency |
Weak association |
Strong association |
Differential diagnoses
Other differential diagnoses are physiological bowing in which improvement in tibial metaphyseal-diaphyseal angle is observed on follow-up avoiding unnecessary X-rays (Park et al., 2019), importantly, stage-1 of BD has one in three chance of healing with follow-up. Other differential diagnoses are skeletal dysplasia and fibular hemimelia.
The association between vitamin D deficiency and blount's disease
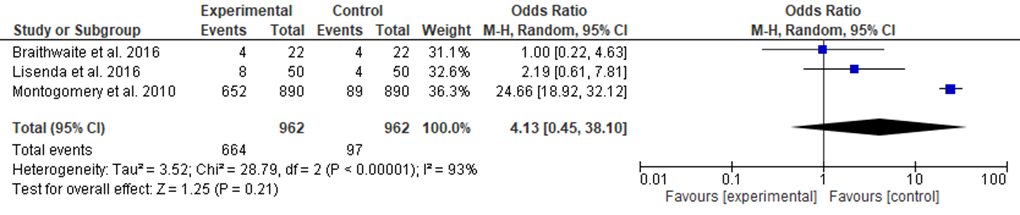
A retrospective study published in the United States concluded the association of vitamin D deficiency with BD. Besides, the association was strong in males with very low vitamin D levels (<16 ng/mL) (Montgomery et al., 2010). A study was conducted in South Africa among fifty patients with BD 30 with infantile, four juvenile, and 16 adolescent. The study showed no differences between BD and the normal population regarding vitamin D status (Lisenda et al., 2016). Another study from Malawi showed no difference between children with rickets and BD regarding vitamin D level (Braithwaite et al., 2016). The author found a low calcium level leading to secondary hyperthyroidism and low phosphate level.
Blount disease and vitamin D deficiency Meta-analysis
MATERIALS AND METHODS
We searched the PubMed, Cochrane Library, and Google Scholar for recent trends in varus deformities; in addition, we searched the grey literature and screened the references of the included studies. The keywords " Varus deformities", "Blount disease", "rickets", "vitamin D deficiency", were used with protean "AND and OR". We identified 245 articles, of them eight full text were screened, and only three evaluated the association of Blount disease and vitamin D deficiency and were eligible for meta-analysis., other studies were included in a narrative review. The studies pooled in the meta-analysis included 1924 patients and 1661 events.
RESULTS AND DISCUSSION
No association between vitamin D deficiency and BD (odds ratio, 4.13, 95% CI, 0.45-38.10, P-value, 0.21). However, the small number of the study included and considerable heterogeneity limited our results (I2 =93%, Chi-square, 28.79, and df=2). Also, we compared vitamin D status with that in the general population in the studies countries when no face-to-face comparison is available (Mastala et al., 2013; Kija et al., 2019). Figure 1. The contradicting results might be explained by the different cut-off values used (16 versus 30 nmol/L). Also, the former study assessed obese children and the later study group was overweight.
|
|
|
Figure 1. Blount disease and vitamin D deficiency |
Obesity, and Obstructive Sleep Apnea and Postoperative Complications
Obstructive sleep apnea among patients with Blount's disease is underdiagnosed despite the grave post-surgical complications including arrhythmia, atelectasis, and respiratory failure. The primary driver of these complications is obesity, which may be present in 100% of patients (Jardaly et al., 2020). Importantly, the associated sarcopenia may add greatly to the suffering of patients with the disease The association between diabetes mellitus, hypertension, and hypothyroidism were also reported (Bowen et al., 2009; Taussig et al., 2016; Kadowaki et al., 2017; Aly et al., 2020).
CONCLUSION
Blount disease (BD) is a great mimlcker of rickets. However, no association was found between the disease and vitamin D deficiency.
ACKNOWLEDGMENTS: The authors would like to acknowledge the Saudi Digital library for accessing the data.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Abdul, N. S. (2021). Teledentistry application during covid -19 pandemic in Saudi Arabia: An overview. Annals of Dental Specialty, 9(1), 13-15.
Abdulsahib, W. K., & Abood, S. J. (2021). The effect of Calcium channel blocker in the Betamethasone-induced Glaucoma model in rabbits. Journal of Advanced Pharmacy Education and Research, 11(1), 135-140.
Aly, W. W., Mohamed, A. H., Farid, T. M., Mortagy, A. K., & Saad, W. E. S. (2020). Prevalence of Sarcopenia and its relation to Vitamin D in elderly females. Medical Science, 24(103), 1276-1286.
Bhattacharjee, R., Chakraborty, P. P., Roy, A., & Biswas, S. N. (2016). Blount's disease: A rickets mimicker. Case Reports, 2016, bcr2016215682. doi:10.1136/bcr-2016-215682
Bowen, J. R., Assis, M., Sinha, K., Hassink, S., & Littleton, A. (2009). Associations among slipped capital femoral epiphysis, tibia vara, and type 2 juvenile diabetes. Journal of Pediatric Orthopaedics, 29(4), 341-344. doi:10.1097/BPO.0b013e3181a53b29
Braithwaite, V. S., Freeman, R., Greenwood, C. L., Summers, D. M., Nigdikar, S., Lavy, C. B. D., Offiah, A. C., Bishop, N. J., Cashman, J., & Prentice, A. (2016). The aetiology of rickets-like lower limb deformities in Malawian children. Osteoporosis International, 27(7), 2367-2372. doi:10.1007/s00198-016-3541-7
Chotigavanichaya, C., Salinas, G., Green, T., Moseley, C. F., & Otsuka, N. Y. (2002). Recurrence of varus deformity after proximal tibial osteotomy in Blount disease: Long-term follow-up. Journal of Pediatric Orthopaedics, 22(5), 638-641.
de Pablos, J., Arbeloa-Gutierrez, L., & Arenas-Miquelez, A. (2018). Update on treatment of adolescent Blount disease. Current Opinion in Pediatrics, 30(1), 71-77. doi:10.1097/MOP.0000000000000569
DMTS, S., & De Leucio, A. (2020). Blount Disease. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK560923/
Ho-Fung, V., Jaimes, C., Delgado, J., Davidson, R. S., & Jaramillo, D. (2013). MRI evaluation of the knee in children with infantile Blount disease: Tibial and extra-tibial findings. Pediatric Radiology, 43(10), 1316-1326. doi:10.1007/s00247-013-2686-1
Huang, Y., Gu, J., Zhou, Y., & Li, Y. (2014). Osteotomy at the distal third of tibial tuberosity with LCP L-buttress plate for correction of tibia vara. Journal of Orthopaedic Surgery and Research, 9(1), 1-9. doi:10.1186/1749-799X-9-9
Jamil, K., Rashid, A. A., & Ibrahim, S. (2015). Tibia vara and slipped upper femoral epiphysis: Is there an association? Journal of Pediatric Orthopaedics B, 24(1), 46-49. doi:10.1097/BPB.0000000000000101
Janoyer, M. (2019). Blount disease. Orthopaedics & Traumatology: Surgery & Research, 105(1), S111-S121. doi:10.1016/j.otsr.2018.01.009
Jardaly, A., McGwin Jr, G., & Gilbert, S. R. (2020). Blount disease and obstructive sleep apnea: An under-recognized association? Journal of Pediatric Orthopaedics, 40(10), 604-607. doi:10.1097/BPO.0000000000001591
Kadowaki, S., Hori, T., Matsumoto, H., Kanda, K., Ozeki, M., Shirakami, Y., Kawamoto, N., Ohnishi, H., & Fukao T. (2017). Prepubertal onset of slipped capital femoral epiphysis associated with hypothyroidism: A case report and literature review. BMC Endocrine Disorders, 17(1), 59. doi:10.1186/s12902-017-0210-6
Khanfour, A. A. (2012). Does langenskiold staging have a good prognostic value in late onset tibia vara? Journal of Orthopaedic Surgery and Research, 7(1), 23. doi:10.1186/1749-799X-7-23
Kija, E., Gidal, B. E., Shapson-Coe, A., Cader, S., van der Watt, G., Delport, S., & Wilmshurst, J. M. (2019). Vitamin D abnormalities and bone turn over analysis in children with epilepsy in the Western Cape of South Africa. Seizure, 69, 186-192. doi:10.1016/j.seizure.2019.04.020
Kohnen, D., Witte, H. D., Sermeus, W., & Schaufeli, W. B. (2021). Studying the relationship between nurses' burnout and the empowering behaviors of nursing leaders. Journal of Integrative Nursing and Palliative Care, 2, 8-13.
LaMont, L. E., McIntosh, A. L., Jo, C. H., Birch, J. G., & Johnston, C. E. (2019). Recurrence after surgical intervention for infantile tibia vara: Assessment of a new modified classification. Journal of Pediatric Orthopaedics, 39(2), 65-70. doi:10.1097/BPO.0000000000000933
Langenskiold, A. (1952). Tibia vara (osteochondrosis deformans tibiae) a survey of 23 cases. Acta Chirurgica Scandinavica, 103, 1-22.
Laoharojanaphand, T., Ariyawatkul, T., Kaewpornsawan, K., Chotigavanichaya, C., Wongcharoenwatana, J., & Eamsobhana, P. (2019). Medial metaphyseal slope as a predictor of recurrence in Blount disease. Orthopaedic Surgery, 11(3), 474-480. doi:10.1111/os.12491
Li, Y., Spencer, S. A., & Hedequist, D. (2013). Proximal tibial osteotomy and Taylor Spatial Frame application for correction of tibia vara in morbidly obese adolescents. Journal of Pediatric Orthopaedics, 33(3), 276-281. doi:10.1097/BPO.0b013e31828800fe
Lisenda, L., Simmons, D., Firth, G. B., Ramguthy, Y., Kebashni, T., & Robertson, A. J. (2016). Vitamin D status in Blount disease. Journal of Pediatric Orthopaedics, 36(5), e59-e62. doi:10.1097/BPO.0000000000000607
Mastala, Y., Nyangulu, P., Banda, R. V., Mhemedi, B., White, S. A., & Allain, T. J. (2013). Vitamin D deficiency in medical patients at a central hospital in Malawi: A comparison with TB patients from a previous study. PLoS One, 8(3), e59017. doi:10.1371/journal.pone.0059017
Montgomery, C. O., Young, K. L., Austen, M., Jo, C. H., Blasier, R. D., & Ilyas, M. (2010). Increased risk of Blount disease in obese children and adolescents with vitamin D deficiency. Journal of Pediatric Orthopaedics, 30(8), 879-882. doi:10.1097/BPO.0b013e3181f5a0b3
Özkan, A., Atmaca, H., Mutlu, I., Celik, T., Ugur, L., & Kisioglu, Y. (2013). Stress distribution comparisons of foot bones in patient with tibia vara: A finite element study. Acta of Bioengineering and Biomechanics, 15(4), 67-72.
Park, B. K., Park, K. B., Kwak, Y. H., Jin, S., Kim, H. W., & Park, H. (2019). A comparative evaluation of tibial metaphyseal-diaphyseal angle changes between physiologic bowing and Blount disease. Medicine, 98(17), e15349. doi:10.1097/MD.0000000000015349
Pereira‐Santos, M., Costa, P. R. D. F., Assis, A. M. O. D., Santos, C. A. D. S. T., & Santos, D. B. D. (2015). Obesity and vitamin D deficiency: A systematic review and meta‐analysis. Obesity Reviews, 16(4), 341-349. doi:10.1111/obr.12239
Rasheed, A. M., Alhejaily, Y. A., Smaisem, M. S., Alsadhan, N. A., & Al Homoud, H. (2020). Determination of obesity classifications as a factor of comorbidity and their relations with joints involvement among patients with rheumatoid arthritis, king Saud medical city 2019-2020. Medical Science, 24(106), 4558-4565.
Sabharwal, S., & Sabharwal, S. (2017). Treatment of infantile Blount disease: An update. Journal of Pediatric Orthopaedics, 37, S26-S31. doi:10.1097/BPO.0000000000001027
Sanghrajka, A. P., Hill, R. A., Murnaghan, C. F., Simpson, A. H. R. W., & Bellemore, M. C. (2012). Slipped upper tibial epiphysis in infantile tibia vara: Three cases. The Journal of bone and joint surgery. British Volume, 94(9), 1288-1291. doi:10.1302/0301-620X.94B9.28271
Taussig, M. D., Powell, K. P., Cole, H. A., Nwosu, S. K., Hunley, T., Romine, S. E., Iwinski, H., Talwalkar, V., Warhoover, T., Lovejoy, S. A., et al. (2016). Prevalence of hypertension in pediatric tibia vara and slipped capital femoral epiphysis. Journal of Pediatric Orthopaedics, 36(8), 877-883. doi:10.1097/BPO.0000000000000569
Tsibidakis, H., Kanellopoulos, A. D., Sakellariou, V. I., Soultanis, K. C., Zoubos, A. B., & Soucacos, P. N. (2014). The role of Taylor Spatial Frame for the treatment of acquired and congenital tibial deformities in children. Acta Orthopaedica Belgica, 80(3), 419-425.
Vukašinović, Z., Stefanović, B., Šešlija, I., Pavlović, M., & Živković, Z. (2013). Treatment of infantile tibia vara-18-year follow-up: A case report. Srpski arhiv za celokupno lekarstvo, 141(5-6), 390-394. doi:10.2298/sarh1306390v
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.