The second most common urologic malignancy worldwide is bladder cancer. There are two main bladder cancers: the squamous cell carcinomas (SCC), where urinary schistosomiasis is an endemic disease and the transitional cell carcinomas (TCC), which is related to cigarette smoking. Rare types of bladder cancer include small cell carcinoma, primary lymphoma, carcinosarcoma, and sarcoma. The current study aims to determine the Awareness of smoking as a risk factor for bladder cancer among the population in Taif city. this study is a cross-sectional study, and it will be done by the collection of data via a questionnaire containing several questions from doctors. This study will be carried out in Taif city population. This study includes a total of 223 participants who met the inclusion criteria and were included in the final analysis, and 9 participants were excluded because they live outside Al-Taif. From the total sample, the majority were aged between 18 and 39-year-old (70.85%), have a bachelor's degree or higher (71.30%), and (51.1%) were males. In terms of smoking status, 52 (23.32%) were current smokers, 16 (7.17%) were x-smokers, while a large percentage were not smokers 155 (69.51%). For the participants’ knowledge about the risks of smoking, (99.55%) know that smoking can cause lung cancer, (97.76%) know it can lead to heart diseases while only tow-third think that it can lead to bladder cancer. The total smokers (36/52) think that smoking can cause bladder cancer (68.16%) those who think that smoking can cause lung cancer.
INTRODUCTION
The second most common urologic malignancy worldwide is bladder cancer, mainly transitional cell carcinoma, but it is the seventh most common malignancy in men and the seventeenth in women (Nazir et al., 2019; Algarni et al., 2020; Almehmadi et al., 2020). There are two main bladder cancers: the squamous cell carcinomas (SCC), which are more frequently seen in some Middle Eastern and African countries, where urinary schistosomiasis is an endemic disease and the transitional cell carcinomas (TCC), which is related to cigarette smoking and is most prevalent in Western and industrialized countries. Rare types of bladder cancer include small cell carcinoma, carcinosarcoma, primary lymphoma, and sarcoma (Gowing et al., 2015). Smoking is the single greatest factor responsible for the development of bladder cancer, followed by extensive occupational exposure to arylamines and causes about 50% and 31% of cases in men and women, respectively (Moradi-Lakeh et al., 2015; Algabbani et al., 2018; Chang et al., 2021). In general, smokers have an increased risk of bladder cancer development when compared to non-smokers, which depends on the number of consumed cigarettes (Nuryunarsih et al., 2021). A prospective observational study was done and the results showed that only 118 of 202 patients (58.4%) stated that they knew that the risk factor for bladder cancer is smoking, as opposed to 94.6, 91.6, and 92.1% who stated that smoking is also related to lung cancer, heart, and vascular problems, and chronic obstructive pulmonary disease (Lam et al., 2007). A cross-sectional study was done and results were with regard to respondent perceptions of smoking as a risk factor for bladder, lung cancer, and renal. 36% of the sample reported that smoking was a risk factor for bladder cancer and 32% reported that smoking was a risk factor for renal cancer compared to 98% who reported that smoking was a risk factor for lung cancer (Terres et al., 1994).
A cross-sectional survey was done and the result reported that the most respondents (74%) had a history of cigarette use and response rate was 70% (344 of 492 eligible participants). 17% of all respondents were diagnosed to be smoking. Smokers with a new diagnosis of bladder cancer were almost 5 times likely to stop smoking in the general population (48% v 10%). The advice of the urologist and the bladder cancer diagnosis led to most of the cessation. When the urologist was the source of their understanding, respondents were more likely to endorse smoking as a risk factor for bladder cancer (Godtfredsen et al., 2008).
Aims/Objectives of the study
The current study aims to determine smoking awareness as a risk factor for bladder cancer in Taif city, KSA.
MATERIALS AND METHODS
Work plan: This study will be divided into several phases as follows:
Phase 1: Optimization of sample collection and sampling.
Phase 2: Data collection.
Phase 3: Computer analysis and writing the research.
Methodology: Cross-sectional study through online surveys manuscript.
Hypothesis: Smokers Males and females are not aware of the association between bladder cancer and smoking. Inclusion criteria: Male and female smokers at any age. Exclusion criteria: non-smoker population outside Taif city. Sample size: At least 200 samples for a confidence level of 95% and a confidence interval of 5%. Analysis plan: Data will be analyzed using SPSS version 23.0 (SPSS, Inc, Chicago, IL, USA).
RESULTS AND DISCUSSION
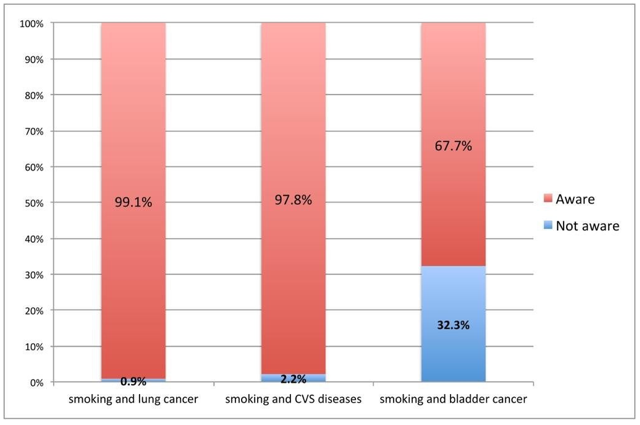
The study was done to assess the awareness of the relationship of smoking with lung cancer, cardiovascular diseases, and bladder cancer, which included 232 participants who gave consent to participate. The participant's sociodemographic characteristics showed that 69.8% were from the age group 18-39 years, 19.4% from 40-49 years, 9.1% from 50- 59 years, and the remaining 1.7% belonged to 60 years and above. The gender distribution showed that 47.8% were females and 52.2% were male participants. The educational qualification of the participants showed that 69.8% had a graduate degree and 0.9% had a Master's degree. In this study, 23.3% reported that they are current smokers, and 7.8% were previous smokers (Table 1). The awareness regarding the relationship between smoking and lung cancer was in this study was found to be 99.1% (n=230) (Figure 1). When we assessed the relationship of this awareness with different baseline characteristics of the participants, there was no statistically significant association observed with age (p=0.728), gender (p=0.174), educational level (p=0.929), and smoking status (p-0.635) (Table 2). The awareness regarding the relationship between smoking and CVS diseases was about 97.8% (n=227) (Figure 1). The assessment of the relationship of this relationship with various baseline characteristics of the participants showed that there was no statistically significant association observed except with the smoking status. Participants who had never smoked were comparatively more aware of this relationship of smoking with CVS diseases (99.4%) than current smokers (98.1%) and previous smokers (83.3%) (Table 3). The assessment of awareness of the relationship between bladder cancer and smoking showed that only 67.7% (n=157) were aware of this (Figure 1). When we compared this awareness with various baseline characteristics, there was no statistically significant association observed with age (p=0.205), gender (p=0.381), educational qualification (p=0.152), and smoking status (p=0.976) (Table 4). When we analyzed the source of this information about the awareness of these relationships, it was found that social media or the Internet was the most common source (31.5%), followed by information from doctors or other health professionals (27.2%), from school or college (21.6%), television (6.5%) from personal experience (6%), journal or magazines or medical textbooks (4.7%) (Figure 1).
Table 1. Baseline characteristics of the participants
|
|
Frequency |
Percent |
|
|
Age |
18-39 |
162 |
69.8 |
|
40-49 |
45 |
19.4 |
|
|
50-59 |
21 |
9.1 |
|
|
60 and more |
4 |
1.7 |
|
|
Gender |
Female |
111 |
47.8 |
|
Male |
121 |
52.2 |
|
|
Educational Qualification |
Primary |
2 |
0.9 |
|
Middle school |
12 |
5.2 |
|
|
High school |
54 |
23.3 |
|
|
Graduate |
162 |
69.8 |
|
|
Masters |
2 |
0.9 |
|
|
Smoking status |
Never-smoker |
160 |
69.0 |
|
Previous smoker |
18 |
7.8 |
|
|
Current Smoker |
54 |
23.3 |
|
Table 2. Association of awareness regarding smoking and lung cancer with various baseline characteristics
|
|
Relationship of smoking and lung cancer |
Total |
P value |
|||
|
Not aware |
Aware |
|||||
|
Age (in Years) |
18-39 |
N |
1 |
161 |
162 |
0.728 |
|
% |
0.6 |
99.4 |
69.8 |
|||
|
40-49 |
N |
1 |
44 |
45 |
||
|
% |
2.2 |
97.8 |
19.4 |
|||
|
50-59 |
N |
0 |
21 |
21 |
||
|
% |
0.0 |
100.0 |
9.1 |
|||
|
60 and more |
N |
0 |
4 |
4 |
|
|
|
% |
0.0 |
100.0 |
1.7 |
|||
|
Gender |
Female |
N |
0 |
111 |
111 |
0.174 |
|
% |
0.0 |
100.0 |
47.8 |
|||
|
Male |
N |
2 |
119 |
121 |
||
|
% |
1.7 |
98.3 |
52.2 |
|||
|
Education al level |
Primary |
N |
0 |
2 |
2 |
0.929 |
|
% |
0.0 |
100.0 |
0.9 |
|||
|
Middle school |
N |
0 |
12 |
12 |
||
|
% |
0.0 |
100.0 |
5.2 |
|||
|
High school |
N |
0 |
54 |
54 |
||
|
% |
0.0 |
100.0 |
23.3 |
|||
|
Graduate |
N |
2 |
160 |
162 |
||
|
% |
1.2 |
98.8 |
69.8 |
|||
|
Masters |
N |
0 |
2 |
2 |
||
|
% |
0.0 |
100.0 |
0.9 |
|||
|
Smoking |
Non- smoker |
N |
2 |
158 |
160 |
0.635 |
|
% |
1.3 |
98.8 |
69.0 |
|||
|
Previous smoker |
N |
0 |
18 |
18 |
||
|
% |
0.0 |
100.0 |
7.8 |
|||
|
Smoker |
N |
0 |
54 |
54 |
||
|
% |
0.0 |
100.0 |
23.3 |
|||
Table 3. Association of awareness regarding smoking and CVS diseases with various baseline characteristics
|
|
Relationship of smoking and CVS diseases |
Total |
P- value |
|||
|
Not aware |
Aware |
|||||
|
Age (in years) |
18-39 |
N |
4 |
158 |
162 |
0.608 |
|
% |
2.5 |
97.5 |
69.8 |
|||
|
40-49 |
N |
0 |
45 |
45 |
||
|
% |
0.0 |
100.0 |
19.4 |
|||
|
50-59 |
N |
1 |
20 |
21 |
||
|
% |
4.8 |
95.2 |
9.1 |
|||
|
60 and more |
N |
0 |
4 |
4 |
||
|
% |
0.0 |
100.0 |
1.7 |
|||
|
Gender |
Female |
N |
1 |
110 |
111 |
0.208 |
|
% |
0.9 |
99.1 |
47.8 |
|||
|
Male |
N |
4 |
117 |
121 |
||
|
% |
3.3 |
96.7 |
52.2 |
|||
|
Educational level |
Primary |
N |
0 |
2 |
2 |
0.978 |
|
% |
0.0 |
100.0 |
0.9 |
|||
|
Middle school |
N |
0 |
12 |
12 |
||
|
% |
0.0 |
100.0 |
5.2 |
|||
|
High school |
N |
1 |
53 |
54 |
||
|
% |
1.9 |
98.1 |
23.3 |
|||
|
Graduate |
N |
4 |
158 |
162 |
||
|
% |
2.5 |
97.5 |
69.8 |
|||
|
Masters |
N |
0 |
2 |
2 |
||
|
% |
0.0 |
100.0 |
0.9 |
|||
|
Smoking |
Non-smoker |
N |
1 |
159 |
160 |
<0.001 |
|
% |
0.6 |
99.4 |
69.0 |
|||
|
Previous smoker |
N |
3 |
15 |
18 |
||
|
% |
16.7 |
83.3 |
7.8 |
|||
|
Smoker |
N |
1 |
53 |
54 |
||
|
% |
1.9 |
98.1 |
23.3 |
|||
Table 4. Association of Awareness regarding smoking and bladder cancer with various baseline characteristics
|
|
Relationship of smoking and bladder cancer |
Total |
P value |
|||
|
No |
Yes |
|||||
|
Age (in years) |
18-39 |
N |
46 |
116 |
162 |
0.205 |
|
% |
28.4 |
71.6 |
69.8 |
|||
|
40-49 |
N |
20 |
25 |
45 |
||
|
% |
44.4 |
55.6 |
19.4 |
|||
|
50-59 |
N |
8 |
13 |
21 |
||
|
% |
38.1 |
61.9 |
9.1 |
|||
|
60 and more |
N |
1 |
3 |
4 |
||
|
% |
25.0 |
75.0 |
1.7 |
|||
|
Gender |
Female |
N |
39 |
72 |
111 |
0.381 |
|
% |
35.1 |
64.9 |
47.8 |
|||
|
Male |
N |
36 |
85 |
121 |
||
|
% |
29.8 |
70.2 |
52.2 |
|||
|
Educatio nal level |
Primary |
N |
0 |
2 |
2 |
0.152 |
|
% |
0.0 |
100.0 |
0.9 |
|||
|
Middle school |
N |
7 |
5 |
12 |
||
|
% |
58.3 |
41.7 |
5.2 |
|||
|
High school |
N |
14 |
40 |
54 |
||
|
% |
25.9 |
74.1 |
23.3 |
|||
|
Graduate |
N |
54 |
108 |
162 |
||
|
% |
33.3 |
66.7 |
69.8 |
|||
|
Masters |
N |
0 |
2 |
2 |
||
|
% |
0.0 |
100.0 |
0.9 |
|||
|
Smoking |
Non- smoker |
N |
51 |
109 |
160 |
0.976 |
|
% |
31.9 |
68.1 |
69.0 |
|||
|
Previous smoker |
N |
6 |
12 |
18 |
||
|
% |
33.3 |
66.7 |
7.8 |
|||
|
Smoker |
N |
18 |
36 |
54 |
||
|
% |
33.3 |
66.7 |
23.3 |
|||
|
|
|
Figure 1. Awareness of the relationship between cancer, CVS and smoking |
The prevalence of smoking has dramatically increased worldwide despite the efforts to combat its use through various risk awareness strategies and tobacco control policies (Gowing et al., 2015; Nazir et al., 2019). In Saudi Arabia, reports from two national surveys conducted in the year 2013 (Moradi-Lakeh et al., 2015) and 2018 (Algabbani et al., 2018) have shown that the prevalence of tobacco smoking is found to be 12.2% and 21.4%, respectively, which is alarming and has become a serious public health concern. Smoking increases the risk of many diseases, including pneumonia, cardiac attacks, strokes, chronic obstructive pulmonary disease (COPD) (including emphysema and chronic bronchitis), and several cancers such as lung cancer, oropharyngeal cancers, bladder cancer, and pancreatic cancer. It is also a risk factor for many peripheral arterial diseases and hypertension (Chang et al., 2021; Nuryunarsih et al., 2021). The awareness regarding the health risks of smoking is essential to help smokers to quit and non-smokers not to take up the habit. Quitting smoking at any age is found to have immediate health benefits and also in reducing the risk of lung disorders, cardiovascular diseases, and some smoking-related cancers (Terres et al., 1994; Lam et al., 2007; Godtfredsen et al., 2008). Among smoking-related cancers, lung cancer is one of the leading causes of death in tobacco smokers (Youlden et al., 2008; Cheng et al., 2016). In our study, most of the participants were aware of this relationship. A study conducted by Trofor et al. (2018) among tobacco users in six European reported that awareness of the relationship between smoking and lung cancer was as follows: Germany (89.8%), Greece (96.1%), Hungary (83.4%), Poland (87.4%), Romania (90.2%) and Spain (93.1%). In Saudi Arabia, a study done among medical students reported that only 12.6% of the students knew that the risk of dying from lung cancer reduces to half for a person who stops smoking (Jradi & Al-Shehri, 2014). Another study conducted in the city of Riyadh among medical students showed that 94% of the students were having good knowledge of the relationship between smoking and lung cancer (Al-Haqwi et al., 2010). A study conducted in Iraq reported that 80.6% of smokers were aware of smoking's health risk on lung cancer (Dawood et al., 2016). The pathogenesis behind lung cancer and smoking is not completely defined. The inflammation produced due to cigarette smoke is found to play a major role in carcinogenesis (Prendergast, 2008). Tobacco smoking is found with a 2-4 fold increase in the risk of cardiovascular diseases (CVDs) and greater than 75% excess mortality rate from CVS disease (Lakier, 1992; Nancy et al., 2021). The lack of awareness of the CVDs and their risk factors are important barriers in the prevention and treatment of these diseases. Our study findings showed that 97.8% of the participants were aware of the risk of smoking with CVDs. Despite the awareness, all the smokers (100%) in this study continue to smoke. A recent study done in the city of Riyadh among Saudi citizens showed that approximately 75% of the participants considered smoking as a risk factor for CVDs (Mujamammi et al., 2020). The prevalence of CVDs in Saudi Arabia is rising, and tobacco smokers are at increased risk of suffering from morbidities and mortalities related to it (Alhabib et al., 2020). A study done by Ahmed et al. (2017) found that smoking is a modifiable risk factor for 20% of people having CVDs. It is also evident that involuntary exposure to tobacco smoke (passive smoke) in non-smokers increases the risk of morbidity and mortality from CVDs (Barnoya & Glantz, 2005; US Department of Health and Human Services, 2006). It is estimated that every year throughout the world, more than 350,000 people are diagnosed with bladder cancer (Bray et al., 2018). Despite the clear evidence of the presence of numerous carcinogenic compounds in cigarette smoke, it is one of the second leading causes of mortality in cancer patients (Bray et al., 2018). There is authentic evidence that tobacco smoking is an important risk factor for developing bladder cancer (Zeegers et al., 2000; Simonis et al., 2014). Our study findings showed the awareness regarding the relationship between bladder cancer and smoking is not that high compared to awareness of the relationship between lung cancer and CVDs. According to a report in 2004, bladder cancer is the most common genitourinary cancer in Saudi Arabia (Abomelha, 2004; Melikov et al., 2021). It is reported that screening for bladder cancer is less compared to other cancers, which could be related to the overall low incidence compared to other smoking-related cancers (Krabbe et al., 2015; Alhussain et al., 2021). It is very clear from researches that smoking is a modifiable risk factor for many diseases, including lung cancer, bladder, and CVDs. The findings of this study show that most participants were aware of the harmful effect of smoking and its relationship with various diseases. Despite the increased awareness, smokers continue to smoke, and there is a need to understand different barriers to quit smoking. It is imperative to know about various risk factors, especially modifiable risk factors, to make better lifestyle choices.
CONCLUSION
This study demonstrated a higher level of awareness regarding smoking and its relationship with lung cancer and coronary heart diseases, but the awareness regarding bladder cancer was moderate among the participants. Efforts should be made to transform this high awareness to encourage positive attitudes towards smoking cessation and lifestyle behavioral changes in smokers. This study's findings would help health policymakers and health care professionals understand the current awareness regarding smoking and its relationship with various diseases. This understanding could be utilized to plan tobacco control policies and other alternative strategies to minimize tobacco usage.
ACKNOWLEDGMENTS: The authors are greatfult to all support and guidance of Dr. Ahmed Fahd Al Thobity.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Abomelha, M. S. (2004). Genito-urinary cancer in Saudi Arabia. Saudi Medical Journal, 25(5), 552-556.
Ahmed, A. M., Hersi, A., Mashhoud, W., Arafah, M. R., Abreu, P. C., Al Rowaily, M. A., & Al-Mallah, M. H. (2017). Cardiovascular risk factors burden in Saudi Arabia: The Africa Middle East cardiovascular epidemiological (ACE) study. Journal of the Saudi Heart Association, 29(4), 235-243.
Algabbani, A. M., Almubark, R., Althumiri, N., Alqahtani, A., & BinDhim, N. (2018). The prevalence of cigarette smoking in Saudi Arabia in 2018. Food and Drug Regulatory Science Journal, 1(1), 1-13.
Algarni, S. B., Alsugair, M. M., Alkhars, M. K., Addas, M. J., Hakeem, M. A., AlSalman, A. A., AlFaresi, Y. R., Alqahtani, A. M., Almalki, A. F., & Alatawi, S. A. S., (2020). Evaluation role of imaging studies in the staging of breast cancer. Archives of Pharmacy Practice, 11(4), 70-75.
Alhabib, K. F., Batais, M. A., Almigbal, T. H., Alshamiri, M. Q., Altaradi, H., Rangarajan, S., & Yusuf, S. (2020). Demographic, behavioral, and cardiovascular disease risk factors in the Saudi population: Results from the Prospective Urban Rural Epidemiology study (PURE-Saudi). BMC Public Health, 20(1), 1213.
Al-Haqwi, A. I., Tamim, H., & Asery, A. (2010). Knowledge, attitude and practice of tobacco smoking by medical students in Riyadh, Saudi Arabia. Annals of Thoracic Medicine, 5(3), 145-148.
Alhussain, B. S., Alfayez, A. A., Alduhaymi, A. A., Almulhim, E. A., Assiri, M. Y., & Ansari, S. H. (2021). Effect of various antibacterial materials in dental composites: A systematic review. Annals of Dental Specialty, 9(3), 39-44.
Almehmadi, M., Alzahrani, K., Salih, M. M., Alsharif, A., Alsiwiehri, N., Shafie, A., Almalki, A. A., Dahlawi, H., Al-hazmi, A., Al-khalidi, A., et al. (2020). Assessment of thyroid gland function by evaluating of TSH, FT3 and FT4 hormones in untreated cancer patients. Journal of Advanced Pharmacy Education & Research, 10(4), 37-42.
Barnoya, J., & Glantz, S. A. (2005). Cardiovascular effects of secondhand smoke: Nearly as large as smoking. Circulation, 111(20), 2684-2698.
Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., & Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A cancer Journal for Clinicians, 68(6), 394-424.
Chang, J. T., Anic, G. M., Rostron, B. L., Tanwar, M., & Chang, C. M. (2021). Cigarette smoking reduction and health risks: A systematic review and meta-analysis. Nicotine and Tobacco Research, 23(4), 635-642.
Cheng, T. Y. D., Cramb, S. M., Baade, P. D., Youlden, D. R., Nwogu, C., & Reid, M. E. (2016). The international epidemiology of lung cancer: Latest trends, disparities, and tumor characteristics. Journal of Thoracic Oncology, 11(10), 1653-1671.
Dawood, O. T., Rashan, M. A. A., Hassali, M. A., & Saleem, F. (2016). Knowledge and perception about health risks of cigarette smoking among Iraqi smokers. Journal of Pharmacy & Bioallied Sciences, 8(2), 146-151.
Godtfredsen, N. S., Lam, T. H., Hansel, T. T., Leon, M. E., Gray, N., Dresler, C., Burns, D. M., Prescott, E., & Vestbo, J. (2008). COPD-related morbidity and mortality after smoking cessation: Status of the evidence. European Respiratory Journal, 32(4), 844-853.
Gowing, L. R., Ali, R. L., Allsop, S., Marsden, J., Turf, E. E., West, R., & Witton, J. (2015). Global statistics on addictive behaviours: 2014 status report. Addiction, 110(6), 904-919.
Jradi, H., & Al-Shehri, A. (2014). Knowledge about tobacco smoking among medical students in Saudi Arabia: Findings from three medical schools. Journal of Epidemiology and Global Health, 4(4), 269-276.
Krabbe, L. M., Svatek, R. S., Shariat, S. F., Messing, E., & Lotan, Y. (2015). Bladder cancer risk: Use of the PLCO and NLST to identify a suitable screening cohort. In Urologic Oncology: Seminars and Original Investigations (Vol. 33, No. 2, pp. 65-e19). Elsevier.
Lakier, J. B. (1992). Smoking and cardiovascular disease. The American Journal of Medicine, 93(1), S8-S12.
Lam, T. H., Li, Z. B., Ho, S. Y., Chan, W. M., Ho, K. S., Tham, M. K., Cowling, B. J., Schooling, C. M., & Leung, G. M. (2007). Smoking, quitting and mortality in an elderly cohort of 56 000 Hong Kong Chinese. Tobacco Control, 16(3), 182-189.
Melikov, I., Kryuchkova, S., Khrapov, S., Otyutskiy, G., & Kryuchkova, E. (2021). Correspondence between society and culture as form and content. Journal of Advanced Pharmacy Education and Research, 11(3), 162-166.
Moradi-Lakeh, M., El Bcheraoui, C., Tuffaha, M., Daoud, F., Al Saeedi, M., Basulaiman, M., Memish, Z. A., AlMazroa, M. A., Al Rabeeah, A. A., & Mokdad, A. H. (2015). Tobacco consumption in the Kingdom of Saudi Arabia, 2013: Findings from a national survey. BMC Public Health, 15(1), 611-621.
Mujamammi, A. H., Alluhaymid, Y. M., Alshibani, M. G., Alotaibi, F. Y., Alzahrani, K. M., Alotaibi, A. B., Almasabi, A. A., & Sabi, E. M. (2020). Awareness of cardiovascular disease associated risk factors among Saudis in Riyadh City. Journal of Family Medicine and Primary Care, 9(6), 3100-3105.
Nancy, A., Sukinah, A., Maram, A., Sara, A., Hiba, A., & Manar, A. (2021). Dental and skeletal manifestation of sickle-cell anaemia and thalassemia in Saudi Arabia; A systematic review. International Journal of Pharmaceutical Research and Allied Sciences, 10(3), 1-7.
Nazir, M. A., Al-Ansari, A., Abbasi, N., & Almas, K. (2019). Global prevalence of tobacco use in adolescents and its adverse oral health consequences. Open access Macedonian Journal of Medical Sciences, 7(21), 3659-3666.
Nuryunarsih, D., Lewis, S., & Langley, T. (2021). Health risks of kretek cigarettes: A systematic review. Nicotine & Tobacco Research.
Prendergast, G. C. (2008). Inflammatory mediators in cancer etiology and targets for therapy and prevention. Cancer Reviews Online, 9, 17-18.
Simonis, K., Shariat, S. F., & Rink, M. (2014). Urothelial cancer working group of the young academic urologists (YAU) working party of the European association of urology (EAU). Smoking and smoking cessation effects on oncological outcomes in nonmuscle invasive bladder cancer. Current Opinion in Urology, 24(5), 492-499.
Terres, W., Becker, P., & Rosenberg, A. (1994). Changes in cardiovascular risk profile during the cessation of smoking. The American Journal of Medicine, 97(3), 242-249.
Trofor, A. C., Papadakis, S., Lotrean, L. M., Radu-Loghin, C., Eremia, M., Mihaltan, F., Driezen, P., Kyriakos, C. N., Mons, U., Demjén, T., et al. (2018). Knowledge of the health risks of smoking and impact of cigarette warning labels among tobacco users in six European countries: Findings from the EUREST-PLUS ITC Europe Surveys. Tobacco Induced Diseases, 16.
US Department of Health and Human Services. (2006). The health consequences of involuntary exposure to tobacco smoke: A report of the surgeon general. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
Youlden, D. R., Cramb, S. M., & Baade, P. D. (2008). The international epidemiology of lung cancer: Geographical distribution and secular trends. Journal of Thoracic Oncology, 3(8), 819-831.
Zeegers, M. P., Tan, F. E., Dorant, E., & van den Brandt, P. A. (2000). The impact of characteristics of cigarette smoking on urinary tract cancer risk: A meta‐analysis of epidemiologic studies. Cancer, 89(3), 630-639.
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.