The observed higher rate of appendectomy despite the success of the conservative (non-surgical) approach might be due to the lack of awareness. The cecal appendix is not merely rudimentary because of its role on the gut microbiota and the host immune system. This meta-analysis aimed to assess the association of appendectomy at baseline with inflammatory bowel diseases. The PubMed, Cochrane library, and Google Scholar databases were systematically searched for relevant articles. The keywords used were inflammatory bowel disease, appendicitis, appendectomy, gut lymphoid tissue, Crohn's disease, ulcerative colitis with protean "AND" or "OR". No limitation was applied to the time of publication. Out of the 622 references found, 32 full texts were screened, and only eight studies fulfilled the inclusion and exclusion criteria. There were fifteen cohorts from eight studies (five were published in Europe, two were from Asia, and one from South America with 9703 participants and 1150 events). The overall effects showed a negative impact of appendectomy on the rate of Crohn's disease, odd ratio, 0.311, 95% CI, 1.20-8.05, P-value = 0.02. In ulcerative colitis and appendectomy arm, appendectomy was protective for ulcerative colitis, odd ratio, 0.44, 95% CI, 0.35-0.55, P-value = 0.001. Significant heterogeneities were observed (95% for Crohn's disease prevalence, P-value <0.001, and Chi-square, 118.69, and 86% for ulcerative colitis arm P-value <0.001, and Chi-square, 51.54). Appendectomy was protective against ulcerative colitis, however, the impact was negative on Crohn's disease. Further studies assessing the effects of appendectomy on the prognosis of ulcerative colitis are recommended.
INTRODUCTION
Inflammatory bowel disease (IBD) is a global disease in the current century, the incidence and prevalence varies widely (Srivastava et al., 2019). An increasing rate is observed in Africa, Asia, and South America (newly industrialized countries), while stability or reduction was found in Europe and North America (Ng et al., 2018). An increasing rate of appendectomy is observed worldwide despite the emergence of a conservative approach, a high rate of negative results were observed (15-30%) due to reliance on clinical judgement (Mundada et al., 2020). In addition, the appendix together with the tonsils contains copious lymphoid tissue (MALTOmas). Furthermore, a cross-talk is thought to exist between the two lymphoid organs and the gut microbiota (Li et al., 2021). The unique architecture of the caecal appendix, its diversity, and content of gut flora suggested a role as a safe house for gut biodiversity (Babakhanov et al., 2021; Jabbar et al., 2021) and not merely a rudimentary. IBD is a chronic immune-mediated chronic inflammatory disease with the complex interaction between environmental factors, and the gut microbiome in a genetically predisposed individual (Alshammari et al., 2019; Zheng & Wen, 2021). Although the etiology of IBD remained elusive, a multifactorial (genetic predisposition and environmental factors) pathogenesis is suggested. An interesting issue is the hygiene hypothesis, which was observed to hold. The assumption is that good hygiene during childhood with a lower infection rate predispose to autoimmune disease (Salgado et al., 2020). The relationship between appendectomy and IBD is complex and controversial. Thus, this meta-analysis was conducted to assess the impact of appendectomy on IBD.
MATERIALS AND METHODS
Eligibility criteria according to PICOS (Liberati et al., 2009)
Among the 622 articles screened, 502 articles remained after the removal of duplication. However, only 32 full texts were eligible and 15 cohorts from eight studies were pooled to assess the relationship of an appendectomy at baseline and inflammatory bowel disease (eight studies investigated ulcerative colitis and seven assessed the relationship between appendectomy and Crohn's disease). Because of the lack of randomized controlled trials, we included retrospective cohorts and case-control studies on humans that were published in English. Case reports, case series, experimental, and animal studies were excluded.
Intervention: Appendectomy at baseline.
Outcome measures: Inflammatory bowel disease, Crohn's disease, or ulcerative colitis at baseline. We did not investigate the temporal profile of the disease.
The search strategy
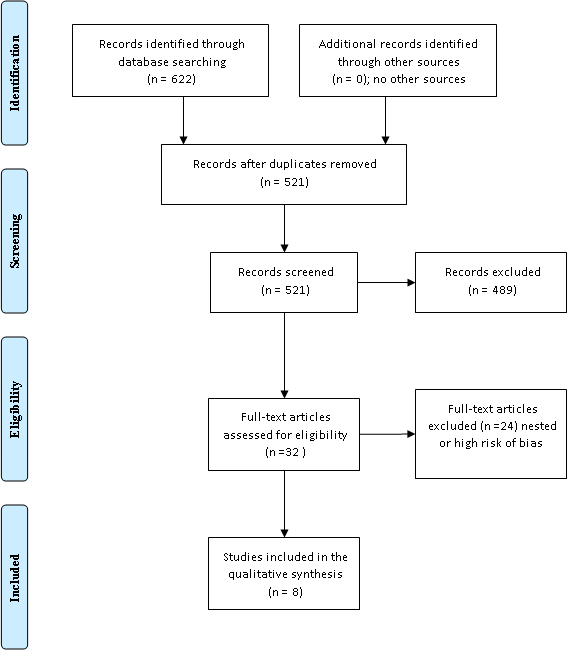
The PubMed, Cochrane library, and Google Scholar databases were systematically searched for relevant articles; the two authors independently screened the titles and abstracts. An additional search was conducted through the references of the retrieved articles. The keywords used were inflammatory bowel disease, appendicitis, appendectomy, gut lymphoid tissue, Crohn's disease, ulcerative colitis with protean "AND" or "OR". No limitation was applied to the time; all studies from the first published up to February 8. 2021 were included. Out of the 622 references found, 32 full texts were screened, and only eight studies fulfilled the inclusion and exclusion criteria. Figure 1 shows different phases of the systematic literature search.
The quality of studies and risk of bias assessment were performed by the Ottawa Newcastle scale for non-randomized studies (Stang, 2010) Table 1.
Statistical analysis
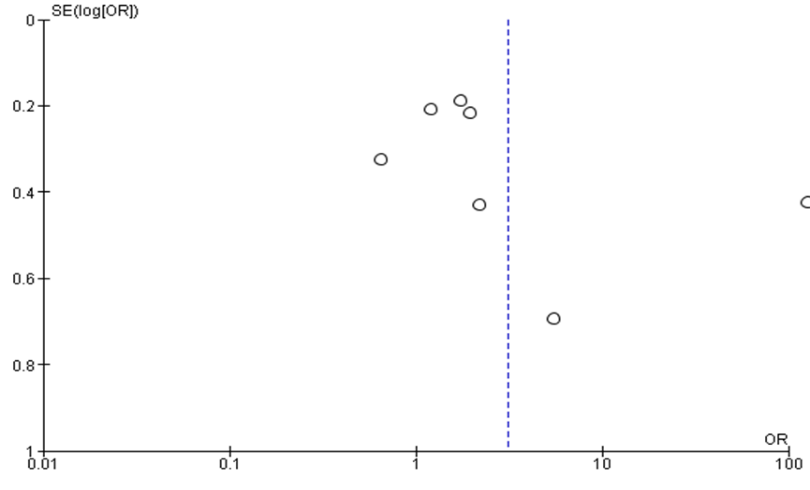
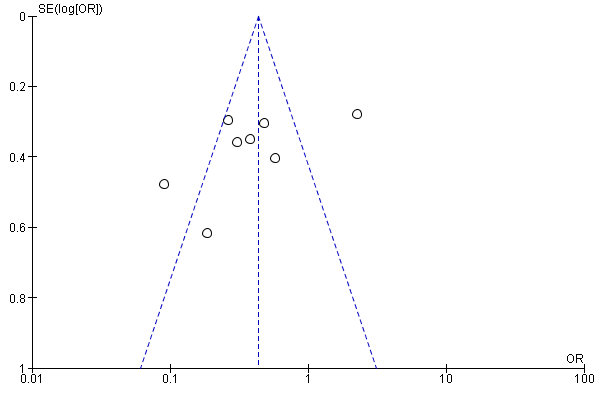
The most recent RevMan version 5.4 was used for data analysis, the data were entered manually at 95% CI. A P-value of <0.05 was considered significant. The random effect was used due to the significant heterogeneity observed (>50%). Funnel plots assessed the sensitivity (lateralization of the included studies).
|
|
|
Figure 1. Appendectomy association with inflammatory bowel disease (The PRISMA Chart) |
Table 1. Ottawa Newcastle assessment for the included studies
|
Author |
Selection |
Compatibility |
Outcome |
Score |
|
Smithson et al., 1995 |
3 |
2 |
4 |
9 |
|
Koutroubakis et al., 1999 |
3 |
2 |
4 |
9 |
|
Reif et al., 2001 |
3 |
2 |
4 |
9 |
|
López Ramos et al. 2001 |
3 |
2 |
4 |
9 |
|
Firouzi et al., 2006 |
3 |
2 |
4 |
9 |
|
Castiglione et al., 2012 |
3 |
2 |
4 |
9 |
|
López-Serrano et al., 2010 |
3 |
2 |
4 |
9 |
|
Sakgado et al., 2020 |
3 |
2 |
4 |
9 |
RESULTS AND DISCUSSION
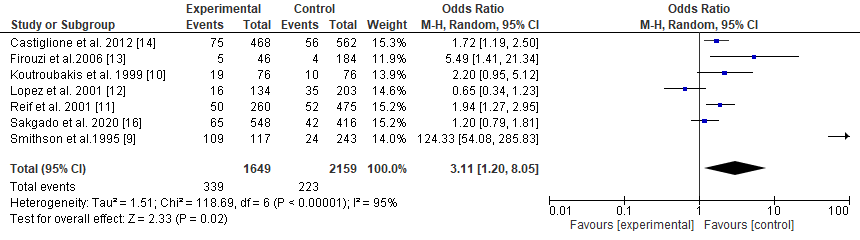
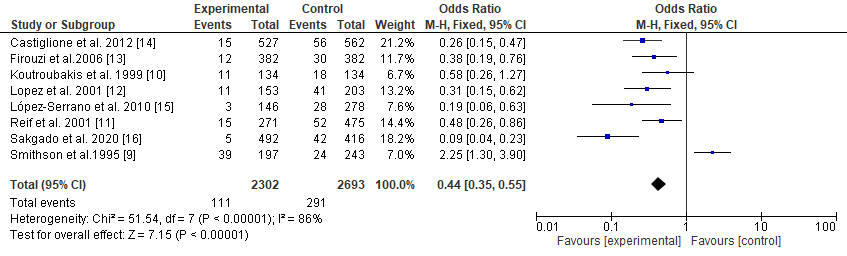
In the present study, fifteen cohorts from eight studies are included (five were published in Europe, two were from Asia, and one from South America), six out of seven cohorts showed a higher rate of Crohn's disease among appendectomy patients and one reported a lower prevalence (3808 subjects included with 658 events). However, the overall effects showed a negative effect of appendectomy regarding the rate of Crohn's disease, odd ratio, 0.311, 95% CI, 1.20-8.05, P-value = 0.02. In ulcerative colitis and appendectomy arm (5895 and 492 events), one study showed lower appendectomies among the control group (Smithson et al., 1995), while the rest showed the reverse (Koutroubakis et al., 1999; López-Ramos et al., 2001; Reif et al., 2001; Firouzi et al., 2006; López-Serrano et al., 2010; Salgado et al., 2010; Castiglione et al., 2012; AlAssad et al., 2021). The results implied that appendectomy was protective for ulcerative colitis, odd ratio, 0.44, 95% CI, 0.35-0.55, P-value = 0.001. Significant heterogeneities were observed (95% for Crohn's disease prevalence, P-value <0.001, and Chi-square, 118.69, and 86% for ulcerative colitis arm P-value, <0.001, and Chi-square, 51.54,). The random effect was applied due to significant heterogeneities (Table 2, Figures 2 and 3).
Table 2. The relationship of appendectomy and inflammatory bowel disease
|
Author |
Country |
Methodology |
Crohn's disease |
Ulcerative colitis |
Control group |
|
Smithson et al., 1995 |
UK |
Case-control |
109/ 117 |
39/197 |
24/243 |
|
Koutroubakis et al., 1999 |
Greece |
Case-control |
19/76 |
11/ 134 |
18/134 U, 10/76 C |
|
Reif et al., 2001 |
Israel |
Case-control |
50/ 260 |
15/ 271 |
52/475 U, 52/475 C |
|
López Ramos et al., 2001 |
Spain |
Case-control |
16/134 |
11/153 |
41/203 U, 35/203 C |
|
Firouzi et al., 2006 |
Iran |
Case-control |
5/46 |
12/382 |
30/382 U, 4/184 |
|
Castiglione et al., 2012 |
Italy |
Retrospective |
75/468 |
15/527 |
56/562 |
|
López-Serrano et al., 2010 |
Spain |
Case-control |
|
3/146 |
28/278 |
|
Sakgado et al., 2020 |
Brazil |
Case-control |
65/548 |
256/492 |
42/416 |
|
|
|
a) |
|
|
|
b) |
|
Figure 2. The effects of appendectomy on Crohn’s disease |
|
|
|
a) |
|
|
|
b) |
|
Figure 3. The impact of appendectomy on the rate of Ulcerative colitis |
In the present review, appendectomy was lower among patients with ulcerative colitis in agreement with a previous study that included nineteen studies assessing both the risk of developing ulcerative colitis and the time course of the disease in addition to appendiceal orifice inflammation (Deng & Wu, 2016). The current analysis assessed both ulcerative colitis and Crohn's disease. Another study searched MEDLINE and found an increased risk of Crohn's disease in similarity to the current findings. However, the previous findings were limited by the heterogeneity observed (Kaplan et al., 2008; Chanda & Aluru, 2021). A meta-analysis published more than two decades ago and limited by gathering information from articles with different methodologies (reviews, conferences, and abstracts) concluded the inverse relationship between appendectomy and ulcerative colitis (Koutroubakis & Vlachonikolis, 2000). The present study was limited by the heterogeneity, but it is among the best recent pieces of evidence to show the inverse relationship between appendectomy and ulcerative colitis and the negative impact on Crohn's disease.
Environment and inflammatory bowel disease
Recent literature found that the first-generation migrants maintained the inflammatory bowel disease risk of their naïve country and convergence to the destination on subsequent generations. Acquiring the risk of inflammatory bowel disease was stronger with the earlier age at migration suggesting a substantial influence of environmental socio-economic factors (Fiorino et al., 2021). Various environmental factors are to blame in the pathogenesis of IBD, one of the crucial steps is the influence of the gut microbiota on the peroxisome proliferator-activated receptors (PPARγ). Impaired expression of the latter enzyme was observed among patients with ulcerative colitis (Caioni et al., 2021). Other factors include antibiotic use, air pollution, infections, diets, and other lifestyles (Shouval & Rufo, 2017).
A wider look at appendectomy and ulcerative colitis
The question that needs to be addressed is the use of appendectomy as a treatment of ulcerative colitis. A meta-analysis published in the USA showed that appendectomy might increase the rate of subsequent colectomy (Parian et al., 2017). These findings supported the findings from a Korean study (Lee et al., 2015). Further meta-analyses found that appendectomy in the established disease was associated with a higher rate of dysplasia and colorectal cancer (Stellingwerf et al., 2019). The above findings together with the observation that appendicular orifice inflammation did not influence the course of ulcerative colitis questioned the use of appendectomy as a treatment for ulcerative colitis.
The study was limited by the significant heterogeneity observed, the limitation to the English language, and the unlimited period of the included studies.
CONCLUSION
Appendectomy might protect against ulcerative colitis and negatively affect Crohn's disease.
ACKNOWLEDGMENTS: The authors acknowledge the Saudi Digital Library for accessing the data.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
AlAssad, F., Alqhtani, N., & Alshammery, D. (2021). Implementation of teledentistry in postgraduate dental education during COVID-19 pandemic in Saudi Arabia. Annals of Dental Specialty, 9(1), 20-26.
Alshammari, R. M., Alhussain, S. M., Al Fateel, Z. A., Al Wtayyan, H. A., Muammar, M. F. B., Alhussain, A. M., Alskaker, B. A., Alahmed, A. M., Alharbi, A. S., Aldhafeeri, S. S., et al. (2019). Evaluation of recent surgical updates in the management of ulcerative colitis: A simple literature review. Archives of Pharmacy Practice, 10(3), 25-28.
Babakhanov, A. T., Dzhumabekov, A. T., Zhao, A. V., Kuandykov, Y. K., Tanabayeva, S. B., Fakhradiyev, I. R., Nazarenko, Y., & Saliev, T. M. (2021). Impact of appendectomy on gut microbiota. Surgical Infections, 22(7), 651-661. doi:10.1089/sur.2020.422
Caioni, G., Viscido, A., d’Angelo, M., Panella, G., Castelli, V., Merola, C., Frieri, G., Latella, G., Cimini, A., & Benedetti, E. (2021). Inflammatory bowel disease: New insights into the interplay between environmental factors and PPARγ. International Journal of Molecular Sciences, 22(3), 985. doi:10.3390/ijms22030985
Castiglione, F., Diaferia, M., Morace, F., Labianca, O., Meucci, C., Cuomo, A., Panarese, A., Romano, M., Sorrentini, I., D'Onofrio, C., et al. (2012). Risk factors for inflammatory bowel diseases according to the “hygiene hypothesis”: A case–control, multi-centre, prospective study in Southern Italy. Journal of Crohn's and Colitis, 6(3), 324-329. doi:10.1016/j.crohns.2011.09.003
Chanda, C., & Aluru, R. R. (2021). Anticuagulants: An overview of natural and synthetic therapeutic anticoagulants. Journal of Biochemical Technology, 12(1), 17-21.
Deng, P., & Wu, J. (2016). Meta-analysis of the association between appendiceal orifice inflammation and appendectomy and ulcerative colitis. Revista Española de Enfermedades Digestivas, 108(7), 401-410. doi:10.17235/reed.2016.4176/2015
Fiorino, G., Estevinho, M. M., Lopes, D. J., Chersi, F., Allocca, M., Souto, M. T., Danese, S., & Magro, F. (2021). Inflammatory bowel disease in migrant populations: Should we look even further back? Current Drug Targets, 22(15), 1706-1715. doi:10.2174/1389450122666210203193817
Firouzi, F., Bahari, A., Aghazadeh, R., & Zali, M. R. (2006). Appendectomy, tonsillectomy, and risk of inflammatory bowel disease: A case control study in Iran. International Journal of Colorectal Disease, 21(2), 155-159. doi:10.1007/s00384-005-0760-3
Jabbar, E. G., Al-Tamimi, D. J. J., Al-Mahroos, M. I. A., Al-Tamimi, Z. J. J., & Ibraheem, J. J. (2021). Pharmacokinetics and bioequivalence study of two formulations of Cefixime suspension. Journal of Advanced Pharmacy Education and Research, 11(1), 170-177.
Kaplan, G. G., Jackson, T., Sands, B. E., Frisch, M., Andersson, R. E., & Korzenik, J. (2008). The risk of developing Crohn's disease after an appendectomy: A meta-analysis. American Journal of Gastroenterology, 103(11), 2925-2931. doi:10.1111/j.1572-0241.2008.02118.x
Koutroubakis, I. E., & Vlachonikolis, I. G. (2000). Appendectomy and the development of ulcerative colitis: Results of a metaanalysis of published case-control studies. The American Journal of Gastroenterology, 95(1), 171-176. doi:10.1111/j.1572-0241.2000.01680.x
Koutroubakis, I. E., Vlachonikolis, I. G., Kapsoritakis, A., Spanoudakis, S., Roussomoustakaki, M., Mouzas, I. A., Kouroumalis, E. A., & Manousos, O. N. (1999). Appendectomy, tonsillectomy, and risk of inflammatory bowel disease. Diseases of the Colon & Rectum, 42(2), 225-230. doi:10.1007/BF02237133
Lee, H. S., Park, S. H., Yang, S. K., Kim, S. O., Soh, J. S., Lee, S., Bae, J. H., Lee, H. J., Yang, D. H., Kim, K. J., et al. (2015). Appendectomy and the clinical course of ulcerative colitis: A retrospective cohort study and a nested case–control study from Korea. Journal of Gastroenterology and Hepatology, 30(3), 470-477. doi:10.1111/jgh.12707
Li, P., Killinger, B. A., Ensink, E., Beddows, I., Yilmaz, A., Lubben, N., Lamp, J., Schilthuis, M., Vega, I. E., Woltjer, R., et al. (2021). Gut microbiota dysbiosis is associated with elevated bile acids in Parkinson’s disease. Metabolites, 11(1), 29. doi:10.3390/metabo11010029
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P., Clarke, M., Devereaux, P. J., Kleijnen, J., & Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Journal of Clinical Epidemiology, 62(10), e1-e34. doi:10.1136/bmj.b2700
López Ramos, D., Gabriel, R., Cantero Perona, J., Moreno Otero, R., Fernández Bermejo, M., & Maté Jiménez, J. (2001). Association of MALTectomy (appendectomy and tonsillectomy) and inflammatory bowel disease: A familial case-control study. Revista espanola de enfermedades digestivas: Organo oficial de la Sociedad Espanola de Patologia Digestiva, 93(5), 303-314.
López-Serrano, P., Pérez-Calle, J. L., Pérez-Fernández, M. T., Fernández-Font, J. M., Boixeda de Miguel, D., & Fernández-Rodríguez, C. M. (2010). Environmental risk factors in inflammatory bowel diseases. Investigating the hygiene hypothesis: A Spanish case–control study. Scandinavian Journal of Gastroenterology, 45(12), 1464-1471. doi:10.3109/00365521.2010.510575
Mundada, A., Vaidya, V., & Lamture, Y. (2020). Anorexia in acute appendicitis: A non-specific factor with significant accuracy in diagnosis. Medical Science, 24(105), 2812-2816.
Ng, S. C., Shi, H. Y., Hamidi, N., Underwood, F. E., Tang, W., Benchimol, E. I., Panaccione, R., Ghosh, S., Wu, J. C., Chan, F. K., et al. (2017). Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. The Lancet, 390(10114), 2769-2778. doi:10.1016/S0140-6736(17)32448-0
Parian, A., Limketkai, B., Koh, J., Brant, S. R., Bitton, A., Cho, J. H., Duerr, R. H., McGovern, D. P., Proctor, D. D., Regueiro, M. D., et al. (2017). Appendectomy does not decrease the risk of future colectomy in UC: Results from a large cohort and meta-analysis. Gut, 66(8), 1390-1397. doi:10.1136/gutjnl-2016-311550
Reif, S., Lavy, A., Keter, D., Broide, E., Niv, Y., Halak, A., Ron, Y., Eliakim, R., Odes, S., Patz, J., et al. (2001). Appendectomy is more frequent but not a risk factor in Crohn’s disease while being protective in ulcerative colitis: A comparison of surgical procedures in inflammatory bowel disease. The American Journal of Gastroenterology, 96(3), 829-832. doi:10.1111/j.1572-0241.2001.03529.x
Salgado, V. C. L., Luiz, R. R., Boéchat, N. L. F., Leão, I. S., do Carmo Schorr, B., Parente, J. M. L., Lima, D. C., Júnior, E. S. S., Silva, G. O. S., Almeida, N. P., et al. (2020). Risk factors associated with inflammatory bowel disease: A multicenter case-control study in Brazil. World Journal of Gastroenterology, 26(25), 3611-3624. doi:10.3748/wjg.v26.i25.3611
Shouval, D. S., & Rufo, P. A. (2017). The role of environmental factors in the pathogenesis of inflammatory bowel diseases: A review. JAMA Pediatrics, 171(10), 999-1005. doi:10.1001/jamapediatrics.2017.2571
Shrivastava, B., Gopaiah, K. V., & Rao, G. S. (2019). Lipid-polymer based Nano particles as a new generation therapeutic delivery platform for ulcerative colitis in vitro/in vivo evaluation. Pharmacophore, 10(4), 15-27.
Smithson, J. E., Radford-Smith, G., & Jewell, G. P. (1995). Appendectomy and tonsillectomy in patients with inflammatory bowel disease. Journal of Clinical Gastroenterology, 21(4), 283-286. doi:10.1097/00004836-199512000-00006
Stang, A. (2010). Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. European Journal of Epidemiology, 25(9), 603-605. doi:10.1007/s10654-010-9491-z
Stellingwerf, M. E., de Koning, M. A., Pinkney, T., Bemelman, W. A., D’Haens, G. R., & Buskens, C. J. (2019). The risk of colectomy and colorectal cancer after appendectomy in patients with ulcerative colitis: A systematic review and meta-analysis. Journal of Crohn's and Colitis, 13(3), 309-318. doi:10.1093/ecco-jcc/jjy163
Zheng, L., & Wen, X. L. (2021). Gut microbiota and inflammatory bowel disease: The current status and perspectives. World Journal of Clinical Cases, 9(2), 321-333. doi:10.12998/wjcc.v9.i2.321
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.