Sinusitis is an inflammation of the sinuses’ mucosal lining. Chronic and acute rhinosinusitis are two types of rhinosinusitis with different causal and quite similar symptoms. Facial pain, congestion, and headache are all symptoms of the conditions among others. Due to the significant presence of this condition in the Saudi community, family doctors should be up to speed on the latest diagnosis, therapy, and complications. We aim to explore the literature which reviews rhinosinusitis, and the correspondent etiology, clinical presentation, risk factors, identification, and/or control of this condition. Article gathering and sorting was performed on the PubMed database, and the resulted chosen papers had underwent a further thorough review. The diagnosis of rhinosinusitis is usually dependent based on the clinician's excellent experience, with the patients’ history and examination serving as the foundation. Diagnosing the causal pathogen is just as important as discerning the patient's other risk factors and comorbidities when it comes to determining the best treatment approach and evading unfavorable outcomes.
INTRODUCTION
Air pockets located in the facial bones and bones of the skull are known as paranasal sinuses. Sinusitis is the swelling of the mucosal lining of those sinuses, the inflammation tends to extend to the lining of nose as it has similar characteristics of the sinuses’ lining. Therefore, the term rhinosinusitis is more accurate. This condition has multiple triggers and heavily influenced by the seasonal changes, with spike in spring and winter (Leung et al., 2020; Wu et al., 2020; Biryukova et al., 2021). Sinusitis is a very common disease that is encountered, almost daily, in family medicine practice, it is the second most common infection to be seen in this field (Worrall, 2011). In Saudi Arabia, a study targeted the pediatric population found that almost 30% of the sample had some sort of chronic sinusitis and positive family history (Alshehri et al., 2021). This paper aims to explore the important aspects of this disease, in order to arm the family practitioner with the needed knowledge ensure the patients’ well-being.
MATERIALS AND METHODS
For the selection of the various articles the PubMed database was employed and the following keys used in the mesh ((“Sinusitis"[Mesh OR "Rhinosinusitis"[Mesh]]) AND (“Diagnosis"[Mesh] OR "Management"[Mesh] OR "Risk factors"[Mesh])). Rhinosinusitis, sinusitis, and the correspondent risk factors, evaluation, management or diagnosis were among the criteria used to select the publications for inclusion. All other publications that did not meet the criteria, since their topic did not contain any of the inclusion criterion results, were eliminated.
Review
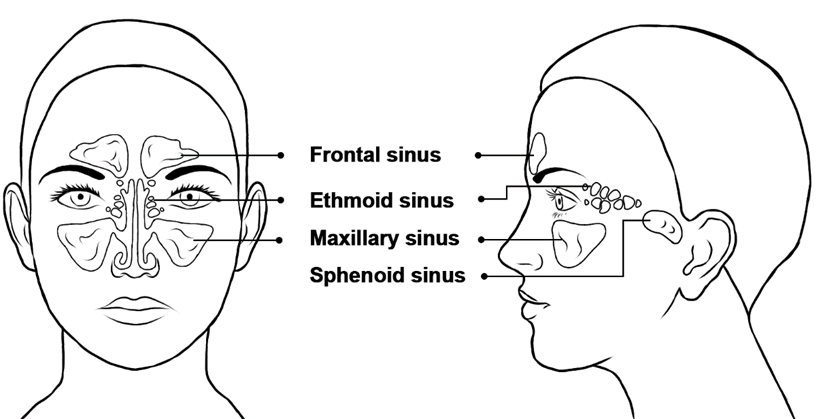
The maxillary, sphenoid, frontal, and ethmoid sinuses are the four paired sinuses, with their names derived from the bone in which it is situated, Figure 1 illustrates the location of each sinus pair. The American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) divides rhinosinusitis into three subgroups based on symptoms duration. Acute rhinosinusitis (ARS) is defined as a sinus infection that lasts less than four weeks, subacute rhinosinusitis is defined as a sinus infection that lasts four to twelve weeks. Moreover, chronic rhinosinusitis (CRS) is a condition when a sinus infection lasts more than twelve weeks. Acute rhinosinusitis can be categorized into viral, bacterial, or even fungal. The main two varieties of chronic rhinosinusitis are chronic rhinosinusitis without nasal polyps (CRSsNP) and the other is with nasal polyps (CRSwNP) (Aring & Chan, 2016).
|
|
|
Figure 1. The four paired paranasal sinuses |
Etiology
As previously mentioned, rhinosinusitis has different etiologies that can present similarly despite their original cause. The most frequent cause of rhinosinusitis is a viral infection (Especially upper respiratory infections), with rhinovirus being the most common culprit. Adenovirus, coronavirus, influenza, parainfluenza viruses, and respiratory syncytial virus are among the other viruses implicated. These viruses attack nasal epithelial cells, causing cell death by disrupting tight junctions and disrupting membranes (Çatlı et al., 2020). Bacterial rhinosinusitis is less commonly present, however, it usually presents as a superinfection on top of a viral one in 0.5–2.0% of cases. However, in bacterial rhinosinusitis, the most conventional pathogens are H. influenzae, , M. catarrhalis, and S. pneumoniae (Patel & Hwang, 2018). When allergic or viral sinusitis strikes the underlying pathophysiology states that , it produces three major alterations in the sinuses system's normal function. The inflammation of the mucosa of the sinuses and oedematous, disrupting mucociliary function by obstructing the sinus ostium. These three changes provide ideal conditions for bacterial growth and proliferation (Aring & Chan, 2016). Different hypotheses were suggested in order to explain chronic rhinosinusitis, widely it is accepted that chronic arises on the ground of one prolonged episode of acute rhinosinusitis. The exact mechanist still vague but tried to be explained multiple models, including: bacteria-based hypotheses, superantigen hypothesis, biofilm hypothesis, microbiome hypothesis, host-related hypotheses, eicosanoid hypothesis, and immune barrier hypothesis (Lam et al., 2015).
Risk factors
Rhinosinusitis is a very complex disease when it comes to risk factors and predisposing conditions. Genetics diseases have their roles in developing these conditions, anatomical anomalies and variation of the maxillofacial structures, primary ciliary dyskinesia, and primary immunodeficiencies, are as well documented disease-related in a significant way to rhinosinusitis. Moreover, comorbid diseases in the patient may exacerbate or harbor rhinosinusitis, researches suggested that atopy, asthma, gastroesophageal reflux, autoimmune/inflammatory diseases, aspirin Sensitivity, and bronchiectasis may have relation in developing this condition. Environmental factors also can initiate a flare such as polluted air and smoking’ due to its effects on ciliary function (Min & Tan, 2015; Tint et al., 2016).
Clinical presentation
The typical two-step approach is advised in assessing rhinosinusitis patients, starting with detailed history. History of any of the following: rhinorrhea, cough, postnasal drip, fever, mucopurulent discharge, recent upper respiratory tract infection, face discomfort, and/or congestion can indicate acute rhinosinusitis. Leaning forward can aggravate facial discomfort, and the location of the pain might indicate which sinus is afflicted. Chronic rhinosinusitis has many of the same symptoms as acute rhinosinusitis, however, with reduced specificity. Headache is a typical complaint among chronic patients, with a sequence that however fades after walking continuously for four hours. And finally, detailed medical history, including family history, is strongly recommended (Evans, 1994; Patel & Hwang, 2018; Çatlı et al., 2020).
Physical examination starts with a general inspection where the typical findings are a watery nose and eyes, pale face, and a reddish nose tip. Followed by specific oronasal examination, both acute and chronic variants have decreased nasal airflow due to injected hyperemic mucosa. Although polyposis may be present in chronic rhinosinusitis, its absence does not rule out the suspicion. The use of a thudichum (nasal) speculum in a general practitioner's setting can offer a very restricted view that required more invasive techniques, provided by rhinoscopy using a flexible or rigid endoscope allows for a more comprehensive vision. When a nasal channel is obstructed, the inferior turbinates become edematous, pale, and watery on both sides. Along with any septal defects and other anatomical variations observed, those findings should be documented and taken into account for the proposed treatment plan (Evans, 1994; Patel & Hwang, 2018; Çatlı et al., 2020).
Diagnosis
Stating a diagnosis of rhinosinusitis is based on the combination of historical findings and physical examination. Table 1 contains the criteria for acute and chronic rhinosinusitis (Rosenfeld et al., 2015; Yudhawati & Yuniawati, 2021). It is recommended to document all episodes, as it will facilitate the management plan and other options to be considered in the future, including referral to a specialist (Evans, 1994). Other laboratory testing and imaging procedure is not initially recommended (Patel & Hwang, 2018).
Table 1. Academy of Otolaryngology-Head and Neck Surgery criteria for rhinosinusitis
|
Acute rhinosinusitis (ARS) |
4 weeks or more of nasal drainage –purulent- (posterior, and/or anterior, and/or both) with facial pain-pressure-fullness, nasal obstruction, and/or both. Purulent nasal discharge is cloudy or colored, opposite to the clear secretions seen with the viral infection. This can be identified either by patient reporting and/or upon examination. Nasal obstruction usually is reported by the patient, with other symptoms like congestion, blockage, stuffiness, and/or found upon examination. Facial pain-pressure-fullness can involve the anterior face, periorbital region, And/or manifest as a headache that is localized or diffused. |
|
Viral rhinosinusitis (VRS) |
Assumption of viral rhinosinusitis can be done when signs and symptoms of acute rhinosinusitis are present for less than 10 days without degeneration. |
|
Acute bacterial rhinosinusitis (ABRS) |
Presumption of bacterial rhinosinusitis to be made when: a) In 10 or more days, we tend to see that the signs and symptoms of acute rhinosinusitis are worsening b) Double worsening: that is defined a relief in the symptoms during the 10-day period with the second wave signs and symptoms coming in worse. |
|
Chronic rhinosinusitis (CRS) |
≥ 12 weeks of two or more of the following: • mucopurulent nasal drainage (posterior, anterior, and/or both) • nasal clogging and/or obstruction • facial pressure or pain or fullness • reduced smelling senses. WITH Swelling documented by one or more of the following: • purulent edema and/or mucus in the anterior ethmoid region and/or middle meatus • polyps in the central meatus, and/or nasal cavity • radiographic imaging findings of inflammation evidence in the paranasal sinuses |
Management
The symptoms and underlying cause of rhinosinusitis are both addressed in the treatment strategy. The cornerstone of treatment for ARS is a mix of nasal corticosteroids, decongestion agents, and antibiotics when a bacterial variety is detected. Oral or topical nasal sprays are used to relieve congestion. In comparison to oral formulas, topical formulas give rapid relief and a more potent impact; nevertheless, chronic usage (more than10 days) can cause tachyphylaxis with a rebound nasal mucosa swelling which can be termed rhinitis medicamentosa. As a result, when it comes to long-term usage, the oral version is favored. In the early stages, a nasal corticosteroid (fluticasone propionate) is indicated in an infection of the upper respiratory tract, because it helps to avoid sinusitis, specifically in people with positive rhinovirus. Regarding the duration of corticosteroid -nasal-, treatment should be amid 14 and 21 days. Lastly, antibiotics had better only be used to treat ABRS, with the following regime and medications: Amoxicillin (500 mg) every eight hours for five to seven days OR Amoxicillin/Clavulanate 625 mg every eight hours for five to seven days. Antihistamines, mucolytic drugs, and nasal saline irrigation are further alternatives to considered if treatment-resistant emerged. In chronic rhinosinusitis, nasal corticosteroids are generally used for a long time, with antibiotics only used when there is an acute bacterial exacerbation. Referral is a key skill in family care. Table 2 lists the indications for early and urgent referral for both acute and chronic patients. After more aggressive medicinal management fails, otorhinolaryngologists may entertain surgical options (Masood et al., 2007; Husain et al., 2018; Pham, et al., 2021).
Table 2. Referral criteria for acute and chronic rhinosinusitis
|
Acute rhinosinusitis (ARS) |
Early referral (within one week) |
When symptoms persist despite optimal therapy, especially immunocompromised patients Frequent recurrence (more than four episodes per year) Any anatomical defects (which may cause an obstruction) Any suspicion of malignancy |
|
Urgent referral (within 24 hours) |
Any orbital complications Severe headache in frontal and/or retro-orbital region Swelling of the forehead Septicemia Meningitis or any neurological manifestations |
|
|
Chronic rhinosinusitis (CRS) |
Early referral (within one week) |
Medical remedies have failed. More than 3 infections of sinuses per year Suspected granulomatous disease, fungal illnesses, and/or melanoma. |
|
Urgent referral (within 24 hours) |
Any swelling and/or severe pain in sinus areas, especially immunocompromised patients |
Complications
Bacterial rhinosinusitis complications may be deadly, therefore it's important to discover them as soon as possible. They resulted by either direct erosion of sinuses' walls around the orbit, skull and/or bloodstream spread. Orbital and neurological indicators are among the signs and symptoms to search for, including inflammatory oedema of the eyelids (orbital involvement may or may not be seen), reduced visual acuity, ophthalmoplegia, displaced globe, extreme frontal headache, frontal inflammation, meningitis symptoms, and/or focal neurological symptoms. The orbital difficulties include preseptal cellulitis, orbital abscess, orbital cellulitis, osteomyelitis, subperiosteal orbital abscess. While the intracranial impediments may include one or more of the following: subdural or epidural empyema, brain abscess, cortical thrombophlebitis, meningitis, sagittal and/or cavernous sinus thrombosis (Masood et al., 2007).
CONCLUSION
One of the most frequent illnesses seen in primary care clinics is rhinosinusitis, thence full comprehension by the family practitioner is advised. The variation and underlying cause would be identified after a thorough history and examination. Rhinovirus is the most frequent virus implicated, whereas S. pneumoniae is the most prevalent bacteria. Treatment consists of symptom control and, if applicable, elimination of the underlying cause. Surgical treatments are reserved for chronic cases and have the potential to develop fatal sequelae.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Alshehri, A. M., Assiri, O. A., Alqarni, A. M., Alkhairi, M. A., Alzahrani, M. A., Alshehri, S. H., Alshehri, N. A., & Abouelyazid, A. Y. (2021). Prevalence and clinical presentation of sinusitis in pediatric age group in Aseer, Saudi Arabia. Journal of Family Medicine and Primary Care, 10(6), 2358-2362. doi:10.4103/jfmpc.jfmpc_2433_20
Aring, A. M., & Chan, M. M. (2016). Current concepts in adult acute rhinosinusitis. American Family Physician, 94(2), 97-105.
Biryukova, N. V., Kharina, A. S., Nesterova, N. V., & Malakhovskiy, V. V. (2021). Historical aspects and features of deontology in preventive medicine. Journal of Advanced Pharmacy Education and Research, 11(3), 77-82.
Çatlı, T., Atilla, H., & Miller, E. K. (2020). Acute viral rhinitis. All Around the Nose: Basic Science, Diseases and Surgical Management, 199-202. doi:10.1007/978-3-030-21217-9_23
Evans, K. L. (1994). Diagnosis and management of sinusitis. BMJ. 309(6966), 1415-1422. doi:10.1136/bmj.309.6966.1415
Husain, S., Amilia, H. H., Rosli, M. N., Zahedi, F. D., & Sachlin, I. S. (2018). Management of rhinosinusitis in adults in primary care. Malaysian Family Physician, 13(1), 28-33.
Lam, K., Schleimer, R., & Kern, R. C. (2015). The etiology and pathogenesis of chronic rhinosinusitis: A review of current hypotheses. Current Allergy and Asthma Reports, 15(7), 41. doi:10.1007/s11882-015-0540-2
Leung, A. K., Hon, K. L., & Chu, W. C. (2020). Acute bacterial sinusitis in children: An updated review. Drugs in Context, 9. doi:10.7573/dic.2020-9-3
Masood, A., Moumoulidis, I., & Panesar, J. (2007). Acute rhinosinusitis in adults: An update on current management. Postgraduate Medical Journal, 83(980), 402-408. doi:10.1136/pgmj.2006.054767
Min, J. Y., & Tan, B. K. (2015). Risk factors for chronic rhinosinusitis. Current Opinion in Allergy and Clinical Immunology, 15(1), 1-13. doi:10.1097/ACI.0000000000000128
Patel, Z. M., & Hwang, P. H. (2018). Acute Bacterial Rhinosinusitis. Infections of the Ears, Nose, Throat, and Sinuses. 133-143. doi:10.1007/978-3-319-74835-1_11
Pham, T. V., Huynh, S. V., Dang-Thi, N., & Tran-Chi, V. (2021). Fear of COVID-19 among Vietnamese undergraduates and predictors of their fear. Journal of Biochemical Technology, 12(3), 27-32.
Rosenfeld, R. M., Piccirillo, J. F., Chandrasekhar, S. S., Brook, I., Ashok Kumar, K., Kramper, M., Orlandi, R. R., Palmer, J. N., Patel, Z. M., Peters, A., et al. (2015). Clinical practice guideline (update): Adult sinusitis. Otolaryngology–Head and Neck Surgery, 152(2_suppl), S1-S39. doi:10.1177/0194599815572097
Tint, D., Kubala, S., & Toskala, E. (2016). Risk factors and comorbidities in chronic rhinosinusitis. Current Allergy and Asthma Reports, 16(2), 16. doi:10.1007/s11882-015-0589-y
Worrall, G. (2011). Acute sinusitis. Canadian Family Physician, 57(5), 565-567.
Wu, D., Bleier, B., & Wei, Y. (2020). Definition and characteristics of acute exacerbation in adult patients with chronic rhinosinusitis: A systematic review. Journal of Otolaryngology-Head & Neck Surgery, 49(1):62. doi:10.1186/s40463-020-00459-w
Yudhawati, R., & Yuniawati, E. (2021). Correlation of serum interleukin-6 level and pneumonia severity index score in patient with community-acquired pneumonia. Journal of Advanced Pharmacy Education and Research, 11(3), 58-62.
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.